Irish Cancer Society 2022 Annual Free Conference
Attend in Person or Online
Irish Cancer Society 2022 Annual Free Conference
Attend in Person or Online
1. We recommend that FIT should be used by primary care clinicians to prioritise patients with clinical features of colorectal cancer for referral for urgent investigation
2. We recommend that a FIT threshold of fHb ≥10μg Hb/g should be used in primary care to select patients with lower gastrointestinal symptoms for an urgent referral pathway for colorectal cancer investigation
3. We recommend that patients should not be excluded from referral from primary care for symptoms on the basis of FIT testing alone
4. We suggest that clinicians should follow up patients with no FIT result to encourage them to return a sample or, where the kit has been lost or inadequately submitted, offer a further test
5. We suggest that patients who decline to return a FIT test should be counselled that evaluation of their symptoms is incomplete, and be encouraged to complete their test
6. We suggest that where no FIT result can be obtained, clinicians should use existing national and local guidelines to assess risk of colorectal cancer
7. We recommend that some patients with symptoms of suspected colorectal cancer may be managed in primary care if fHb <10μg Hb/g, and provided appropriate safety netting is in place
8. We suggest that patients with a fHb <10μg Hb/g but with persistent and unexplained symptoms for whom the GP has ongoing clinical concern should be referred to secondary care for evaluation
9. We recommend that safety netting protocols should incorporate advice and strategies for the diagnosis of colorectal and extra-colonic cancer, as well as other serious gastro-intestinal conditions
10. FIT is a triage tool to identify those patients with symptoms of suspected colorectal cancer who should undergo further colorectal investigation
11. We suggest that FIT be utilised for people with iron deficiency anaemia within primary care to inform urgency of referral
12. We suggest referral of patients with persistent / recurrent anorectal bleeding for flexible sigmoidoscopy if fHb <10μg Hb/g
13. There is currently insufficient evidence to recommend variations in the fHb threshold for referral from primary care according to patient related-factors
14. There is currently insufficient evidence to confirm whether diagnostic accuracy is impacted by the type of FIT analyser used
15. There is currently insufficient evidence to recommend including FIT in a risk score with other clinical features to identify patients with symptoms of suspected colorectal cancer
16. We suggest that FIT may be used to stratify adult patients aged younger than 50 years with bowel symptoms suspicious of a diagnosis of colorectal cancer
17. Colonoscopy is considered the standard method of investigation, however other methods of colorectal imaging may be appropriate in some patients
18. We recommend that for patients with symptoms of a suspected diagnosis of colorectal cancer, CT Colonography is equivalent to colonoscopy for detection of colorectal cancer (the choice of modality should be determined by the local expertise and availability)
19. There is currently insufficient evidence to support use of a specific quantitative FIT threshold to recommend the selection of CT Colonography versus colonoscopy
20. On the basis of limited evidence, clinicians and patients consider FIT as an acceptable test for symptomatic colorectal cancer in most circumstances
21. We recommend that services should consider ways of promoting a high proportion of patients to return FIT kits
22. We recommend that clinicians actively prevent discrimination at any stage of the diagnostic pathway as symptomatic FIT testing is rolled out, with a focus on equity of access and application to all patients with lower GI symptoms
23. We recommend that FIT, as a diagnostic triage tool, can be implemented safely at primary care level, and that a programme of education be developed to facilitate implementation of FIT in primary care
FORCE(USA) has compiled resources and information to help people make informed decisions and receive support.
People diagnosed with Lynch syndrome have an increased risk for colorectal, endometrial and other cancers. Options are available for cancer treatment, screening and prevention for people with Lynch syndrome.
https://www.facingourrisk.org/portal/people-with-lynch-syndrome
Prevention Relevance:
Regular bowel screening and aspirin reduce colorectal cancer among patients with LS but extracolonic cancers are difficult to detect and manage. This study suggests that RS reduces morbidity associated with extracolonic cancers.
Another brilliant resource now available for women living with/beyond and with a predisposition to cancer.
Phase 3 live now
-400 women are diagnosed with Uterine cancer every year. 70-80% diagnosed are living with obesity.
Log on to https://thisisgo.ie/?fbclid=IwAR13F4M_K4vkAjBjD__7C7zDvxQdpgWuSW-IQnmA3JX9LePG9QDh9qay_X8 for accurate info.
Bowel cancer deaths can be prevented through the early detection and removal of polyps.
“We want to prevent polyps turning into early-stage cancers,” Bowel Cancer Australia Medical Director, Graham Newstead AM said.
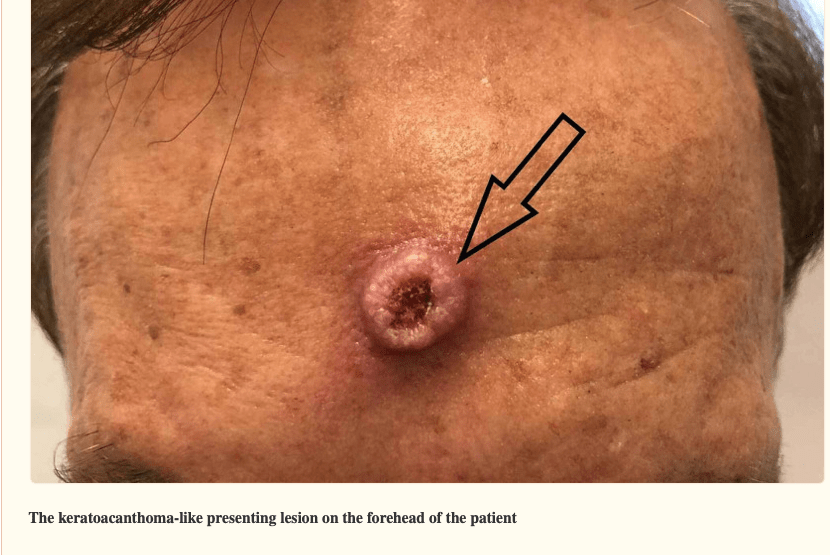
Muir-Torre syndrome (MTS) is a subtype of Lynch syndrome that involves sebaceous neoplasms (e.g., adenoma, carcinoma, epithelioma), keratoacanthomas, or both in addition to other LS-related tumors.
The recommendations from the EHTG and ESCP for identification of patients with Lynch syndrome, colorectal surveillance, surgical management of colorectal cancer, lifestyle and chemoprevention in Lynch syndrome that reached a consensus (at least 80 per cent) are presented.
https://academic.oup.com/bjs/article/108/5/484/6287132?login=false
While there is no diet or workout plan that can cure or prevent cancer, research has shown that a change in eating habits could improve outcomes….
https://www.curetoday.com/view/eat-your-veggies-diet-plays-a-role-in-cancer-occurrence-and-outcomes