ABSTRACT
https://link.springer.com/article/10.1007/s10689-026-00540-9
Highlights
•Germline P/LP variants occur in 10% to 15% of urothelial cancers, up to 20% in UTUC.
•Lynch syndrome is the leading hereditary cause; MSH2 confers the highest risk.
•MMR-deficient tumors, seen in Lynch, are highly sensitive to immune checkpoint inhibition.
•Tumor MMR screening is imperfect and limited by scarce tissue in UTUC biopsies.•Universal germline testing in UTUC and a bladder cancer framework are overdue
https://www.sciencedirect.com/science/article/abs/pii/S1470204526002159?dgcid=coauthor
Information can be found here….
Irish Cancer Society Website:
https://www.cancer.ie/cancer-information/cancer-types/lynch-syndrome
HSE Website:
At the end of last year, Prof Risteárd Ó Laoide stepped down as National Director, a role he had held since 2020.
HSE response to vacancy -“…. Recruitment for senior leadership positions within the HSE follow established human resources policy and procedures. These include a transparent and competitive process, undertaken in line with public sector recruitment standards and governance requirements.”
What about forward planning and having a replacement in place shortly after if not before the handover?
Meanwhile, the Irish Cancer Society’s pre-Budget submission has urged the Government to “prioritise” a new national cancer strategy. The current strategy expires at the end of this year.
“This requires a clear role for the National Cancer Control Programme, and sustained, multi-annual investment in cancer services, infrastructure, and prevention,” according to the submission. It also calls for measures to alleviate the financial hardship of a cancer diagnosis.
Is there anyone in charge of Planning in the HSE???
Home screening test to detect signs of bowel cancer:
https://www2.hse.ie/conditions/bowel-screening/home-screening
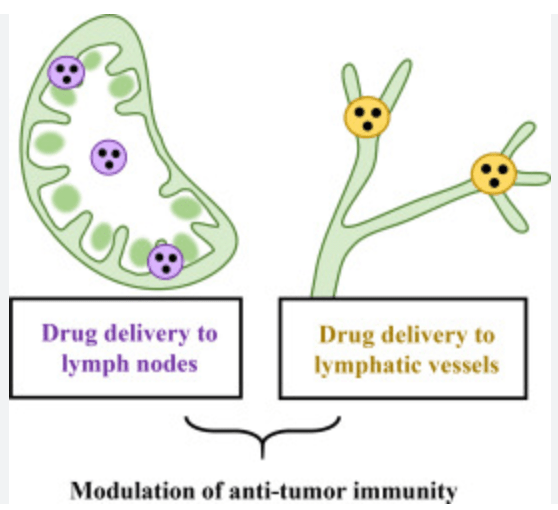
Immunotherapy given before surgery has changed the way many patients with a specific type of bowel cancer (called dMMR colorectal cancer) are treated. Studies show that these medicines can completely destroy cancer in the bowel and nearby lymph nodes in many patients. This suggests that lymph nodes are not just places where cancer spreads, but also play an important role in helping the immune system recognise and attack cancer cells.
However, standard scans are not very good at showing how well immunotherapy has worked. Lymph nodes can remain enlarged because of inflammation caused by the immune response, even when all the cancer has been eliminated. This means scans may suggest cancer is still present when it is not. To make the best treatment decisions, doctors need to combine scan results with other information, such as endoscopy, tissue analysis, and newer tests like blood-based tumour DNA (ctDNA).
These limitations are important because inaccurate scan results could lead to unnecessary surgery or more intensive treatment than a patient actually needs. Researchers are developing better ways to assess treatment response, including advanced imaging and blood tests, to distinguish active cancer from immune-related changes.
For now, surgery with removal of nearby lymph nodes remains the standard treatment for patients with operable dMMR colon cancer. In rectal cancer, avoiding surgery may be possible for some patients who have a complete response to immunotherapy, but only after careful assessment in experienced centres. Whether surgery or lymph node removal can be safely reduced in more patients remains an important question for future research. As more evidence becomes available, a better understanding of how the immune system interacts with lymph nodes may allow treatment to become less invasive while maintaining excellent cancer outcomes.
Pamela’s story is a powerful reminder that your intuition is a vital medical tool. She proved that even when the odds are stacked against you, a new life is possible.
https://untilallsurvive.com/cancer-patients-portraits/pamela-deasy-pancreatic-cancer-ireland