
The study was small (just 21 people), but it builds on a vast body of evidence linking regular exercise to a decreased risk of cancer, particularly colorectal cancer. But the MD Anderson researchers went a step further, investigating how exercise might lower cancer risk.
Category: Colon
Novel Stool RNA Test More Sensitive for Detecting Colon Cancer Versus FIT

The novel multitarget stool RNA test (ColoSense) showed high sensitivity for detecting colorectal neoplasia(new, uncontrolled growth of cells) among adults ages 45 and older, according to the phase III prospective CRC-PREVENT trial.
NCCN guidelines

Genetic/Familial High-Risk Assessment: Colorectal
- NCCN Guidelines Version 1.2023
– Adenomatous Polyposis Testing Criteria
– Attenuated Familial Adenomatous Polyposis
– Colonic Adenomatous Polyposis of Unknown Etiology
– Familial Adenomatous Polyposis
– Juvenile Polyposis Syndrome
– Lynch Syndrome
– MUTYH-Associated Polyposis
– Peutz-Jeghers Syndrome
– Serrated Polyposis Syndrome
A Guide to Lynch Syndrome

Lynch Syndrome is an inherited condition that increases your risk of developing some cancers, including bowel, womb and ovarian cancer. This is a guide to run through everything you need to know about Lynch.
This guide has been made with input from experts, people with Lynch Syndrome and Ask Eve nurses to provide you with all the information you need when offered testing for, or navigating a diagnosis of, Lynch Syndrome.
We also have an Easy Read guide to Lynch Syndrome, which you can download here
Exercise boosts anti-cancer immunity and reduces inflammation in Lynch Syndrome patients
A study led by our Dr. Eduardo Vilar-Sanchez found that intense aerobic exercise may lower the risk of colorectal cancer in patients with #LynchSyndrome.
Note: there are limitations to the study.
Colonoscopy screening in Lynch syndrome

https://link.springer.com/article/10.1007/s10689-023-00347-y
Evidenced-based modelling studies of gene and gender stratified populations suggest a start age and frequency later and less frequent, for MSH6 and PMS2 variant carriers (35 years and 2–3 yearly). The penetrance of MLH1 and MSH2 variant carriers on the other hand does not allow the later start time at least as agreed in most guidelines. This differential surveillance by gene is now being implemented in various guidelines around the world. Such prescription however needs prudent implementation given variable intragenic and even intravariant penetrance estimates in large studies. Note that the confidence intervals in these estimates is relatively large.
There is still the “here and now” which needs to engage carriers and optimize adherence to whatever scheduling is prudent and advised.
How do we do this?
First, registries. Registries keep track of carriers, can provide automated time alerts for the need to attend scheduling ….Registries save lives.
Secondly, patient navigators. Time and time again it has been shown that navigators personally chaperone carriers through the complexities of the healthcare system, to actually reach colonoscopy. They are worth their cost-benefit weight in gold at least in the syndromic scenarios we are discussing.
Thirdly, a pleasant experience helps maintain adherence – the least offensive and effective bowel preparation, a comfortable colonoscopic experience (sedation is important for adherence), and compassionate staff. Efficient throughput (less time for patients) on the day is also valuable. Bowel preparation regime should be personalized against previous experience.
Fourthly, the governance of the risk management service needs to be comprehensive (not just gastrointestinal), patient-centred, interactive with the patient navigators, general practitioners. associated familial cancer clinics (not losing opportunities for time and age appropriate cascade testing across the family), and hospital electronic medical records.
The current study amongst others is important if we are to benefit from the wealth of science that has been uncovered in the understanding of familial cancer. Minimizing the burden of colonoscopies is an important variable, warranting that debate herein described.
Family history of Colorectal cancer – what’s next?

Expert Guest Kevin Monaghan,Gastroenterologist from @StMarksGenomics with an interest in hereditary bowel cancer.
8th UEG Talks #Podcast episode!

http://ueg.eu/podcast Listen to our esteemed host,
@pradeepmundre, and expert guest
New Drug Combo Shows Promising Results Against Early Stages Of Colorectal Cancer
What’s noteworthy about this result is that the patients here, like about 85% of colorectal cancer patients, have what are called “mismatch repair proficient” cancers, which produce highly mutated tumor cells that typically do not respond to immunotherapy. What’s more, Kasi added that based on the results, it may be possible to reduce or even eliminate the need for chemotherapy after surgery, which would otherwise be standard in these kinds of cases.
Lynch Syndrome: Q & A

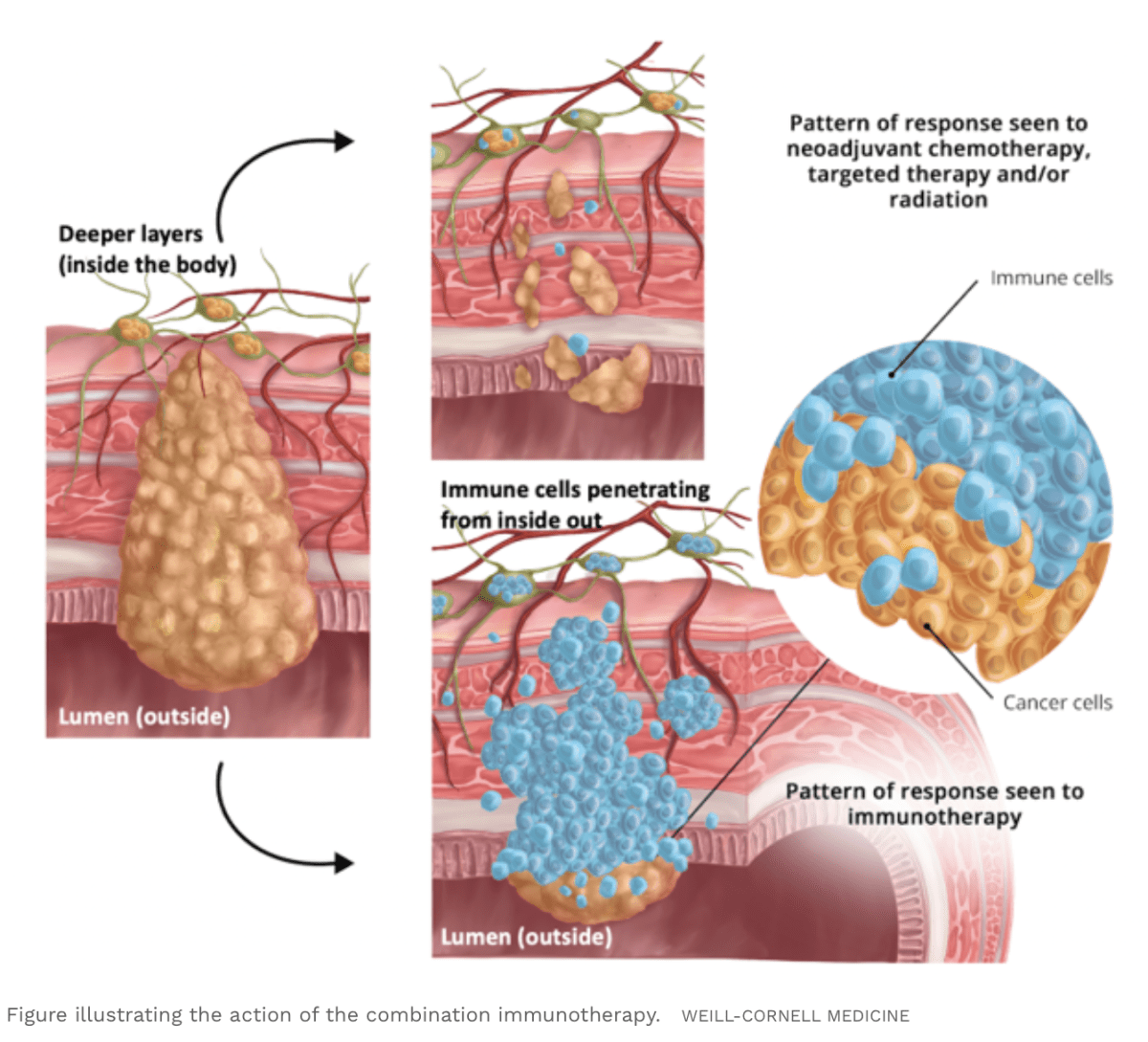
Neoadjuvant Immune Checkpoint Inhibitor Therapy for Localized Deficient Mismatch Repair Colorectal Cancer
Colorectal cancers (CRCs) with deficient DNA mismatch repair (dMMR) account for 15% of all CRCs. Deficient MMR is a predictive biomarker associated with responsiveness to immune checkpoint inhibitors (ICIs) in solid tumors, including CRC. The remarkable effectiveness of ICIs in metastatic CRC has led to their evaluation in the neoadjuvant and adjuvant treatment of localized disease.
Conclusions and Relevance:
While this review found that early results of neoadjuvant immunotherapy for localized dMMR CRC show high rates of major and complete pathological response, longer-term follow-up data are needed to ensure that oncologic outcomes are not compromised and are ideally improved. Neoadjuvant ICI therapy in localized dMMR CRC represents a potential paradigm shift with implications for organ preservation.
https://jamanetwork.com/journals/jamaoncology/article-abstract/2809269
