
This provides the blueprint for the necessary development of hereditary cancer services in Ireland.
Category: Ovarian
Lynch syndrome quick guide for Primary Care clinicians
NCCN: Genetic/Familial High-Risk Assessment: Colorectal (01.2023)

NCCN expanding genetic testing to “Any Lynch related cancer” instead of colon and endometrial cancer as one of the testing criteria
thisisGO.ie is an online personalised resource for you and yours who have been impacted by a gynaecological cancer
The team at thisisGO.ie recognises the importance of having access to the latest scientific research.
See a sample of recent scientific papers pertinent to gynaecological cancers and summaries the key points from each of the papers referenced below.
If this is of interest to you, you can find lots more articles, disease specific, when you “Create a Profile”. Once logged in just search ‘Decoding the Science’.
Lynch syndrome: from detection to treatment

Lynch syndrome is encountered by many clinicians at some stage in their practice and yet remains under-diagnosed with historically limited success in risk stratification and management.
The PLSD(http://plsd.eu) international database continues to expand our knowledge of LS-associated cancer risk. However, we have yet to obtain international consensus on the optimal surveillance strategies, which will be essential among a population of patients who are living beyond their index cancer.
The advent of NGS(next generation sequencing) into clinical practice will undoubtably improve detection rates and allow for more effective, precise, and personalised management programmes for patients with LS.
Finally, over the next decade it will be exciting to see improvements in the preventative strategies that can be offered to patients in the form of aspirin, or even anti-cancer vaccines, as we continue to attempt to disrupt the natural history of this prevalent cancer predisposition syndrome.
Diagnosis and management of Lynch syndrome
https://fg.bmj.com/content/13/e1/e80
A personalised approach to lifelong gene-specific management for people with LS provides many opportunities for cancer prevention and treatment.
What surveillance should these patients undergo?
- Colonoscopic surveillance should be performed every 2 years starting at age 25 years for MLH1, or MSH2 pathogenic variant carriers, or age 35 years for MSH6, or PMS2 pathogenic variant carriers.
- Endoscopic lesions can be difficult to recognise due to a high frequency of flat non-polypoid morphology, and high-quality colonoscopy is essential.
- Gynaecological surveillance has no proven benefit.
- Aspirin reduces long-term colorectal cancer (CRC) risk by approximately 50%. Recommended doses include 150 mg ODonce daily or 300 mg ODonce daily for patients with BMIbody mass index >30.
What surgical treatments are recommended?
- Women should be counselled on prophylactic hysterectomy and bilateral salpingo-oopherectomy from age 40 years (MLH1, MSH2 and MSH6 variant carriers).
- There is a gene-specific approach to surgical management of CRC which takes in to account other patient factors.
What systemic oncological treatments are recommended?
- Chemoprophylaxis with daily aspirin for at least 2 years is recommended in patients <70 years old diagnosed with LS to reduce long-term CRC risk.
- Personalised systemic anticancer therapy is feasible for locally advanced or metastatic disease associated with LS, and may respond very well to relatively novel checkpoint inhibition immunotherapy.
Understanding Lynch Syndrome and Associated Cancer Risk: Epidemiology

Lynch syndrome is the most commonly inherited colon cancer syndrome, and it accounts for approximately 3% of all newly diagnosed cases of colorectal cancer.
The genetics of both the tumor and the germline have an important role in the development and diagnosis of Lynch syndrome.
Mortality by age, gene and gender in carriers of pathogenic mismatch repair gene variants receiving surveillance for early cancer diagnosis and treatment:

A report from the prospective Lynch syndrome database: The PLSD(www.PLSD.eu) is a prospective observational study without a control group that was designed in 2012 and updated up to October 2022. Data for 8500 carriers of path_MMR variants from 25 countries were included, providing 71,713 years of follow up.
Interpretation
The current study found low CRC mortality in path_MMR carriers who receive colonoscopy surveillance while some extracolonic cancers were associated with high mortality. Further improvement of survival in LS may require a focus on the prevention and treatment of non-colorectal cancers, likely including approaches based upon the immune response to MSI pre-cancerous lesions and cancers.
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(23)00086-X/fulltext#secsectitle0095
Care after premenopausal risk-reducing salpingo-oophorectomy in high-risk women: Scoping review and international consensus recommendations

CONCLUSIONS
Despite the efficacy of premenopausal RRSO for reducing ovarian cancer risk and improving mortality in high-risk women, many women experience troublesome menopausal symptoms and oophorectomy may have adverse implications for long-term health.
Our panel of international experts has developed evidence-based recommendations for managing vasomotor, sleep, mood, sexual, and genitourinary symptoms and optimising bone and cardiovascular long-term health. Emerging evidence suggests that HRT reduces but does not eliminate the adverse effects of premenopausal oophorectomy. Women and clinicians considering RRSO should be aware of these risks and clinical care should focus on available safe options for symptom management and optimisation of long-term health.
https://obgyn.onlinelibrary.wiley.com/doi/full/10.1111/1471-0528.17511
Lynch Syndrome

Key Points
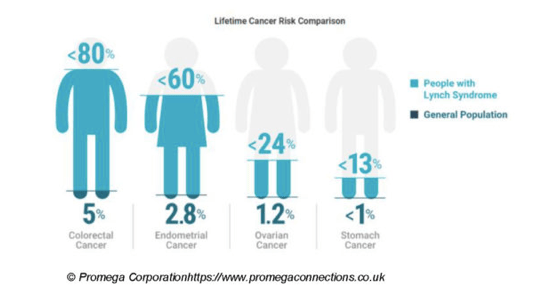
- Lynch syndrome is a rare, inherited condition that increases your risk of developing bowel cancer and sometimes other cancers.
- Lynch Syndrome accounts for about 3% of all bowel cancer.
- Regular bowel screening by colonoscopy can prevent bowel cancers developing.
- Bowel Screening usually starts from the age of 25 years and is performed on a yearly basis.
- People with Lynch Syndrome are also at increased risk of developing certain other cancers such as uterine (womb), urinary tract, ovary and small bowel.
- Women should consider screening of the uterus and ovaries from the age of 30-35 years.
- Genetic testing is available for families with this syndrome.
- When you have Lynch Syndrome, each of your children have a 1 in 2 (50%) chance of inheriting it.
