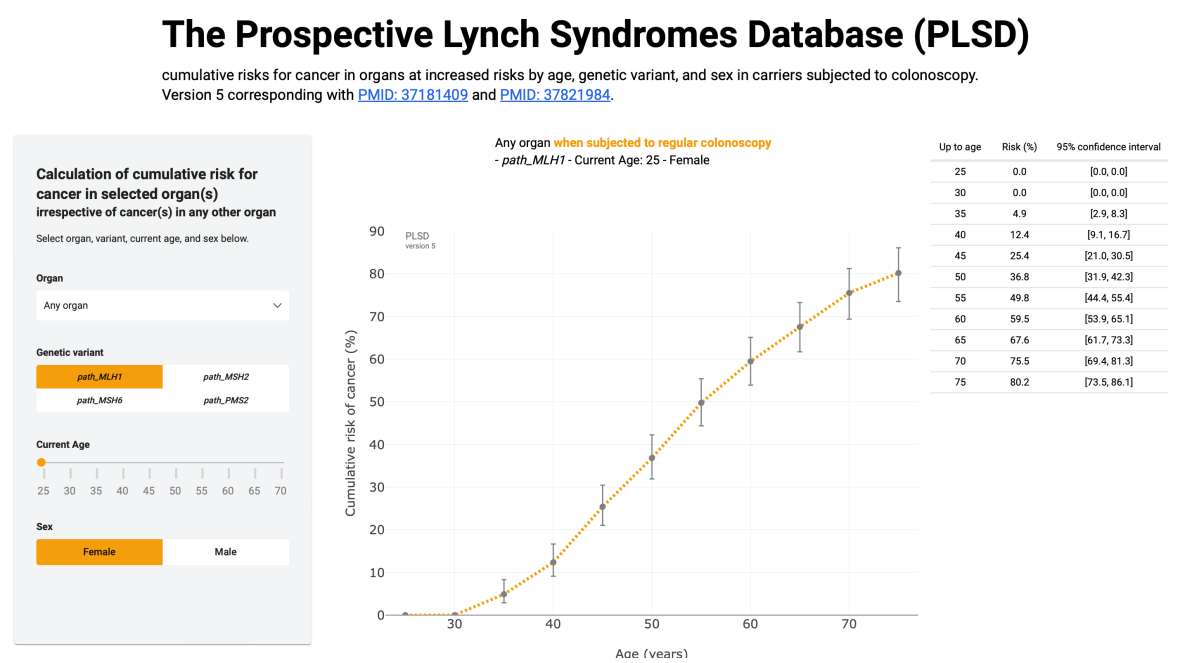
Aims of PLSD
Based on the observation that removal of adenomas with colonoscopy did not reduce CRC incidence as assumed, in 2012 the European Hereditary Tumor Group (EHTG), at that time denoted the Mallorca Group, decided to compile information on follow-up of path_MMR carriers across multiple specialist centres to answer three questions:
- To what degree does colonoscopy surveillance reduce CRC incidence in path_MMR carriers?
- What is the penetrance and expressivity of pathogenic variants in each of the four Lynch syndrome-associated genes?
- What is the survival of carriers when followed-up as recommended, to facilitate early diagnosis and treatment?
path_MMR carriers: Inherited predisposition to colorectal, gynaecological, urinary tract, upper gastrointestinal and other cancers may be caused by pathogenic variants of mismatch repair (path_MMR) genes and commonly referred to as Lynch syndrome.