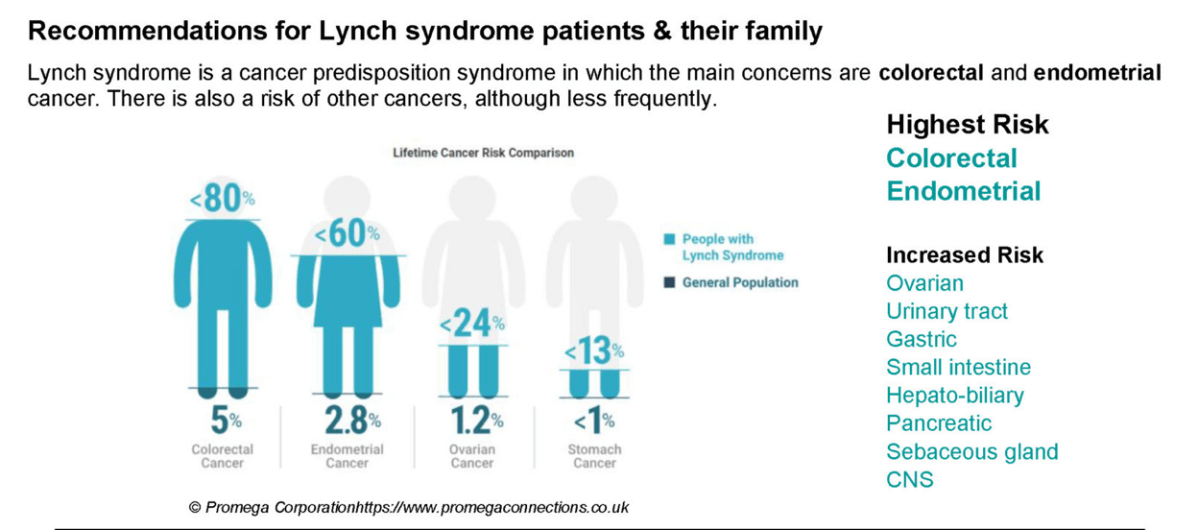
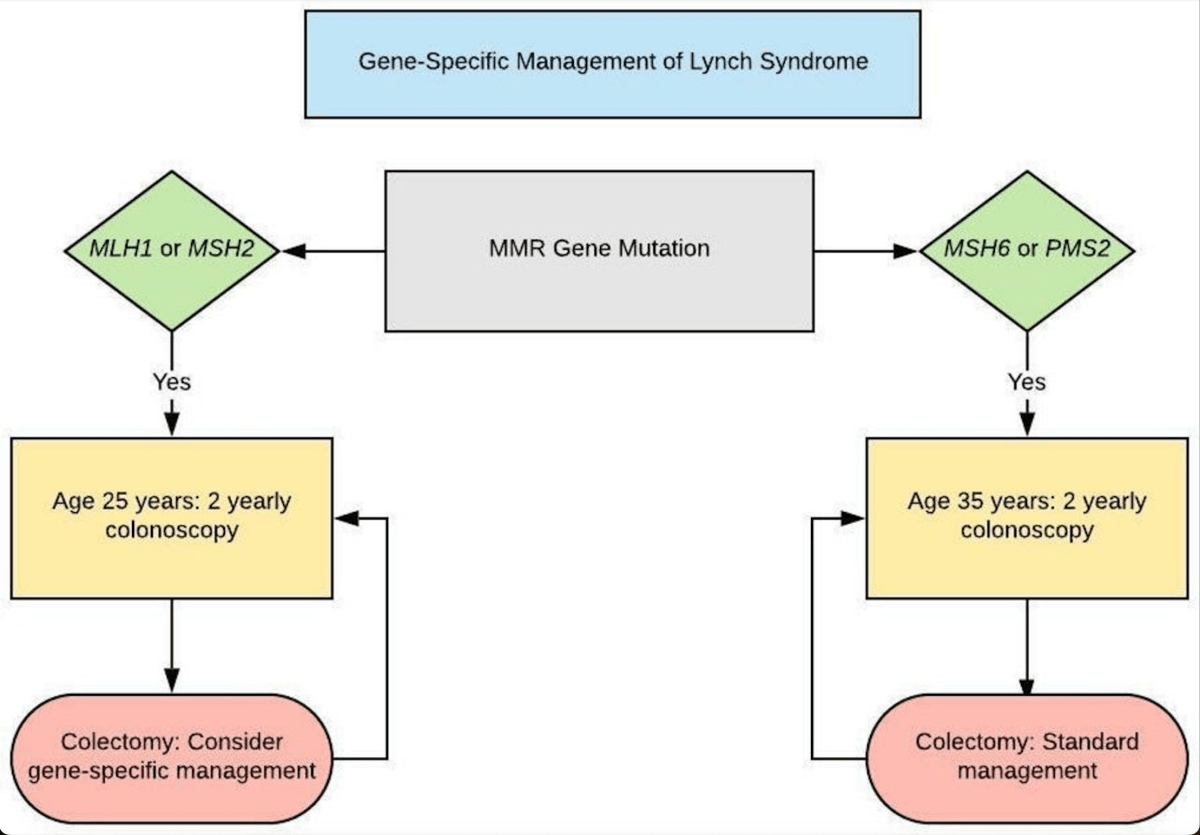
A new Australian study published in The Lancet suggests population-wide genetic screening for hereditary breast and ovarian cancer, familial hypercholesterolemia and Lynch syndrome, in people aged 18 to 40, would be cost effective and save lives.
Modelling demonstrates a marked improvement in the overall cost-effectiveness of offering population genomic screening in a combined fashion for multiple conditions together, versus criteria-based clinical genetic testing or screening for individual conditions.
The model structure can be applied to other healthcare systems, making our findings relevant for international jurisdictions, especially countries with national public healthcare systems capable of delivering nation-wide population screening programs.
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(23)00474-1/fulltext