What’s going on in Lynch Syndrome?
Better way of diagnosing Lynch Syndrome…
Individualising treatment…
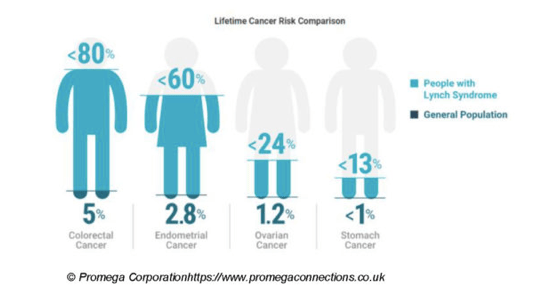
How common is Lynch Syndrome???
No Longer a rare issue.
What’s going on in Lynch Syndrome?
Better way of diagnosing Lynch Syndrome…
Individualising treatment…
How common is Lynch Syndrome???
No Longer a rare issue.
A gene mutation is a change in the genetic instructions in a cell. Genes are the DNA-encoded instructions for building proteins, which are the machinery that does the work inside our cells and our bodies. Some mutations change the function of proteins in ways that increase the risk of cancer or drive its growth.
Gene mutations are not all the same. An understanding of the difference between acquired mutations and inherited mutations can help you make better decisions about cancer care and prevention.
An acquired mutation is acquired during your lifetime.
An inherited mutation is passed down from one or both parents. (These mutations, called germline mutations, can have no effect, be detrimental to health, or be beneficial, or sometimes have both positive and negative effects)
Germline genetic testing identifies inherited mutations. Inherited mutations also tend to be silent until you see a clue, such as a pattern of cancer in your family. If you suspect that you have an inherited mutation, a genetic counselor might suggest germline genetic testing.
Inherited mutations that are associated with cancer don’t directly cause cancer, but they do increase the risk that cancer will develop at some point in a person’s lifetime.
Ireland was the first country in the world to adopt a National Men’s Health Policy, and there were three underlying factors behind the rationale to develop this.
Firstly, there were particular concerns about differences in health outcomes between males and females, and between different groups of males. This led to a call for a specific policy focus on men’s health in Ireland’s National Health Strategy in 2001.
Secondly, there was a recognition of the need to develop a gendered approach to men’s health in order to more effectively engage men in services and programmes.
Thirdly, concerns within wider grass roots men’s health organisations about the state of men’s health, and the health status of specific population groups of men, contributed bottom-up momentum to policy development (Health Service Executive, 2016).
The Men’s Health Forum in Ireland recently launched three publications titled ‘Men’s Health in Numbers’. These tell you everything that you ever wanted to know about the facts and figures on men’s health on the island of Ireland. Download the reports at: https://www.mhfi.org/news/1096-men-s-health-in-numbers.html
‘Research into the methods used in the design, conduct, analysis and reporting of clinical trials is essential to ensure that effective methods are available and that clinical decisions made using results from trials are based on the best available evidence, which is reliable and robust.’
Patient, Public Involvement brings a pragmatism, external perspective and opinions on the uncertainties that methodologists wrestle with as part of the decision making within their work. It is precisely in this space that the contributions can be so valuable. Equally for those us who get involved it provides an opportunity to learn more about health research methods and helps us ask better questions with other projects.
Conclusion: Decision support resources about genetic cancer susceptibility are likely useful to support decision-making…..Tailored patient-facing decision aids should also be made available to patients identified as carriers of a pathogenic gene variant that increases future cancer risks, to complement traditional genetic counselling.
https://www.frontiersin.org/articles/10.3389/frhs.2023.1092816/full
Weird aches and pains abound after cancer treatment, making it hard for patients in remission to figure out whether they’re suffering a treatment side effect or experiencing the first whispers of a cancer recurrence.
“I see patients with different types of cancer and a lot of the time, they want to know ‘Is this pain related to recurrence or is it something else?’” said Fred Hutchinson Cancer Center’s Medical Director of Cancer Rehabilitation Hanna Hunter MD. “In a lot of cases, it’s something else.”
“If you don’t know how to die, don’t worry; Nature will tell you what to do on the spot, fully and adequately. She will do this job perfectly for you; don’t bother your head about it.” – Montaigne
I have been dealing with my mortality for the past 12 years — since I was diagnosed with Lynch syndrome. I struggled with it initially because several family members have died young and have left young children behind.