Category: Monitoring

Family Tree

A genetic history captures details about the health of multiple generations.
This information can be important in diagnosing an inherited condition, revealing a pattern of inheritance, and informing clinical decisions regarding testing and management.
What is a Biomarker?

A biomarker (also called a biological marker) is a piece of information about your health. Biomarkers include your blood pressure, your blood type, and cholesterol or blood sugar levels measured in a blood test. The biomarkers of cancer are also known as tumor markers. Biomarkers can tell your medical team important information about you and your cancer.
Why are biomarkers important?
Colorectal cancer biomarkers can provide your medical team vital information about you and your cancer that is used to determine prognosis, guide treatment decisions, monitor treatment response, and look for recurrence after treatment. Biomarkers are also used in drug development to create and test targeted therapies for colorectal cancer.
Biomarkers of hereditary colorectal cancer
The biomarkers that can confirm hereditary colorectal cancer are the DNA mismatch repair genes causing Lynch Syndrome, and the genes causing Familial Adenomatous Polyposis (FAP) and associated syndromes. Lynch Syndrome is caused by mutations in MLH1, MSH2, MSH3, MSH6, EPCAM, or PMS2 genes, while FAP and other polyposis syndromes are caused by mutations in APC, MYH, BMPR1A, and SMAD4.
From diagnosis of colorectal cancer to diagnosis of Lynch syndrome: The RM Partners quality improvement project

The UK National Institute for Health and Care Excellence recommends universal testing for Lynch syndrome (LS) in all newly diagnosed colorectal cancer (CRC) patients. However, implementation varies significantly by geography. This project was developed to measure variation and deliver an effective diagnostic pathway from diagnosis of CRC to diagnosis of LS (within the RM Partners (RMP) West London cancer alliance).
Conclusion
The LS project was completed by April 2022. We have implemented a systematic approach with workforce transformation to facilitate identification and ‘mainstreamed’ genetic diagnosis of LS. This work has contributed to the development of a National LS Transformation Project in England which recommends local leadership within cancer teams to ensure delivery of diagnosis of LS and integration of genomics into clinical practice.
Lynch Syndrome online training for primary care clinicians
The training involves watching a short video which covers:
- A brief overview of Lynch syndrome
- Their personalised cancer prevention programme
- An introduction to the Lynch syndrome quick guide and how it can help you identify and manage your patient’s care
- How to manage their first-degree family members’ care
The Upsides and Downsides of Cancer Genetic Testing
“Living with a hereditary cancer syndrome inevitably brings uncertainty. Despite taking preventative measures, the knowledge of increased risk frequently lingers in my mind.“
https://www.curetoday.com/view/the-upsides-and-downsides-of-cancer-genetic-testing
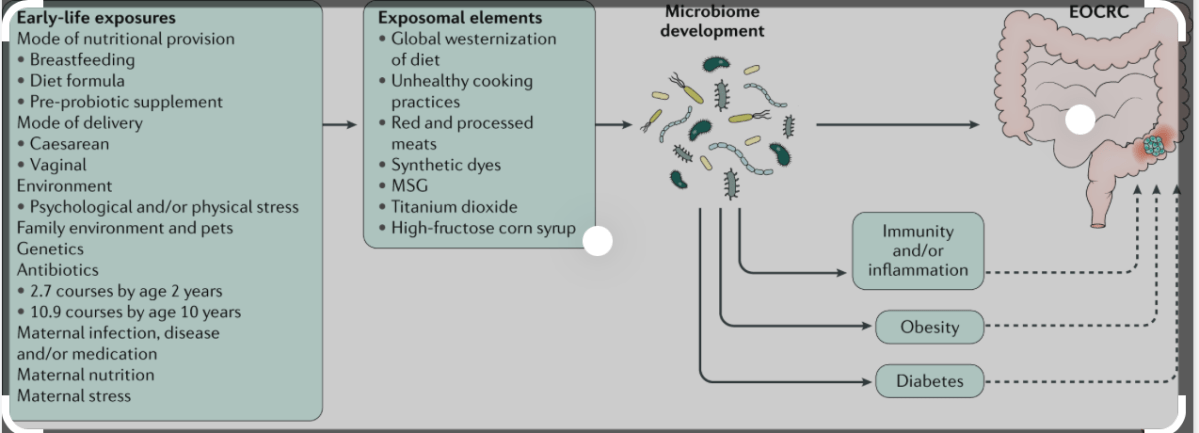
Lights and shadows in the early-onset colorectal cancer management and research: An integrative perspective – Physician scientist with patient advocates
https://www.sciencedirect.com/science/article/pii/S1521691823000318
Practice points
- -The global importance that Early-onset colorectal cancer (EOCRC) is acquiring, makes a joint and worldwide effort necessary to unravel the problem.
- -Although most EOCRC cases seem to be sporadic, there is still an important proportion belonging to families with well-defined colorectal cancer predisposition syndromes.
- –Excluding hereditary syndromes, general population screening strategies don’t cover most cases in the majority of countries, except in some defined ones with first-degree relatives with colorectal cancer.
- -At present, the management of EOCRC should be considered a lifelong process: from the early care of symptoms to avoiding delays in diagnosis; through a multidisciplinary treatment in both the present and future; and with considerations for the possible consequences in the short and long term.
- -The participation of patients in each step of the process, as well as in the awareness of the problem is especially critical in EOCRC.
“How to set up an in-house nurse-led colorectal Lynch syndrome clinic”

In this paper, Filipe Carvalho goes through how he set- up his service, and outlines the essential steps to consider when setting up and managing an in-house nurse-led colorectal Lynch syndrome clinic.
The NHS long term plan sets a target that by 2028, 75% of cancers will be diagnosed at an early stage. One of the ways this ambition will be reached is through targeted screening and personalised surveillance of those most at risk of developing cancer, such as those with Lynch syndrome.
It highlights the educational requirements, patient criteria, the importance of thorough planning and the need to liaise-on with key stakeholders.
https://www.magonlinelibrary.com/doi/abs/10.12968/gasn.2023.21.6.22
Baseline Features and Reasons for Nonparticipation in the Colonoscopy Versus Fecal Immunochemical Test in Reducing Mortality From Colorectal Cancer (CONFIRM) Study, a Colorectal Cancer Screening Trial
The Colonoscopy Versus Fecal Immunochemical Test in Reducing Mortality From Colorectal Cancer (CONFIRM) randomized clinical trial sought to recruit 50 000 adults into a study comparing colorectal cancer (CRC) mortality outcomes after randomization to either an annual fecal immunochemical test (FIT) or colonoscopy.
Conclusions and relevance: In this cross-sectional analysis of veterans(enrollment was through 46 Department of Veterans Affairs medical centers, comprised veterans aged 50 to 75 years with an average CRC risk and due for screening). choosing nonenrollment in the CONFIRM study, those who declined participation more often preferred FOBT or FIT over colonoscopy. This preference increased over time and was strongest in the western US and may provide insight into trends in CRC screening preferences.
The English National Lynch Syndrome Transformation Project

There is consistent evidence of the cost-effectiveness and clinical benefit of a structured diagnostic pathway in patients with LS following a diagnosis of cancer linked to cascade testing in families.
Existing guidelines recommend universal testing of newly diagnosed colorectal and endometrial cancer for Lynch syndrome.
….Another approach to deliver effective diagnosis is to develop ‘mainstreaming’ models whereby patients are offered constitutional genetic testing by their cancer treating teams locally, rather than relying on referral of eligible patients to tertiary services such as clinical genetics.
Conclusions
Whilst there is increased awareness of the cancer risks associated with LS, and other aspects of the condition, by clinicians, there remain significant gains which can be made in diagnosis and subsequent lifelong management of people with LS.
Effective diagnosis needs to deliver people with this condition to effective clinical risk mitigation through a range of mechanisms including nationally coordinated and quality-assured colonoscopic surveillance.
In this project, we have aimed to develop expertise within cancer teams across England, with clear responsibilities, leadership from within which will ensure that the patients they are managing with cancer will receive appropriate testing and delivery diagnosis.
The responsibility for managing cascade testing remains with specialist genomics services.
However lifelong care of people diagnosed with this condition depends on awareness of who this population is, as defined through a national registry, and access to regional multidisciplinary expertise.
https://www.bsg.org.uk/service-success-stories/the-english-national-lynch-syndrome-transformation-project/
