The NordICC trial was a randomized, pragmatic study that enrolled 84,585 adults aged 55 to 64 years old from Poland, Norway, and Sweden.
[T]he NordICC trial … fills an important knowledge gap and provides new insight into the real-world population-wide benefit of colonoscopy for colorectal cancer screening.
Preventing Colorectal Cancer
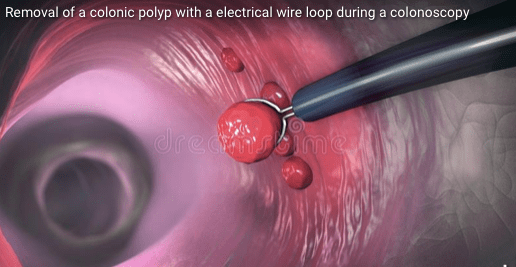
It is important to highlight an advantage of colorectal cancer screening that distinguishes it from all other cancer screening modalities. Colorectal cancer screening with endoscopy is unique in that it aims to, in part, prevent disease by identifying and removing premalignant lesions.
https://ascopost.com/news/november-2022/the-nordicc-trial-the-devil-is-in-the-details/