The prevention of colorectal cancer through colonoscopy relies on identifying and removing adenomas, the main precursor lesion. Nevertheless, colonoscopy is not an optimal strategy since post-colonoscopy colorectal cancer remains an important issue.
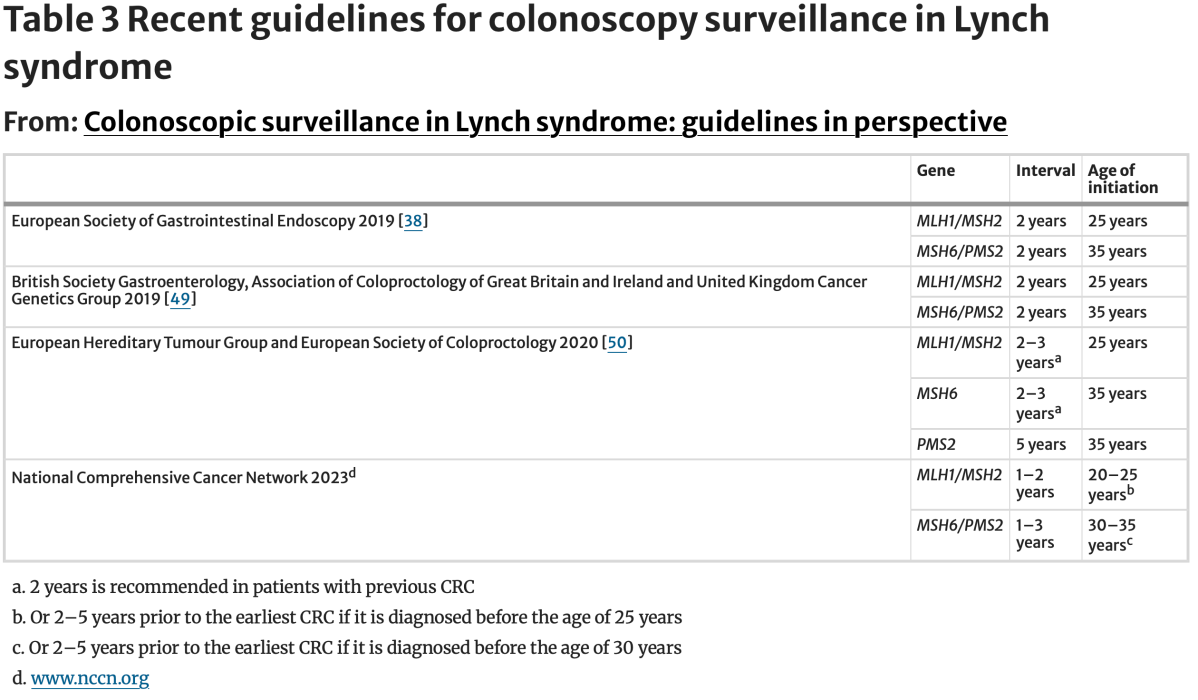
LS is currently understood as a four clinically distinct syndromes with consistent genotype-phenotype associations. Since CRC lifetime risk varies depending on the mismatch repair gene involved, screening guidelines are evolving to become gene specific.
Despite recent advancements, the definitive role of colonoscopy in LS has yet to be established. Current evidence of the variable effect of colonoscopy effectiveness depending on quality indicators in LS suggests that the full potential of colonoscopy has not been achieved.
The coming years are going to be very exciting with the results of the CAPP-3 study that will establish the role of different doses of ASA as cancer prevention, as well as the results of the first trials evaluating the effectiveness and safety of preventive vaccines in LS
https://link.springer.com/article/10.1007/s10689-024-00414-y#Abs1