If you are in Dublin over the coming weeks, please call to @BreakthroCancer#CancerRevolution exhibition which opens today.
Read the inspiring stories, get to see what is being done in #research.
1/2 of us will get a #cancer diagnosis
If you are in Dublin over the coming weeks, please call to @BreakthroCancer#CancerRevolution exhibition which opens today.
Read the inspiring stories, get to see what is being done in #research.
1/2 of us will get a #cancer diagnosis
A recent survey reveals the extent of the issue: 75% of EOCRC patients saw at least two doctors before receiving a diagnosis, and 20% saw four or more. These delays, often driven by medical bias, can be life-altering.
A free online course in Randomised Trials and Their Role in Modern Healthcare! – No prior knowledge needed – At your own pace and takes approximately 5 hours – This course is free to access on FutureLearn Learn more/enrol at:
https://www.futurelearn.com/courses/randomised-trials-and-their-role-in-modern-healthcare
When we attend to both the story and the body that tells it, we move beyond treating disease. We accompany people. We don’t just understand symptoms — we begin to understand lives.
Illness lives in the body — and so does the story of it. You can hear it in a pause before someone answers. You can see it in the way they shift in a chair, the tightness in a jaw, the way breath catches or slows. These are not incidental details. They are part of the narrative, carrying meaning that lab results and scan reports can’t capture.
This is embodied storytelling: when words and the body work together to communicate the lived experience of health and illness.
https://journalofethics.ama-assn.org/article/narrative-embodiment-and-health/2025-06
Is there anyone responsible for figuring this out, or is the whole system just going to drift into the future?
Overall, the National Development Plan is not heavy on specifics. While it refers to the Government’s commitment to health digitalisation, there is no detail.
As regards healthcare, more detail and a clearer sense of long-term ambition will be essential if this plan is to deliver meaningful and lasting reform.
Colonoscopy is expected to reduce colorectal cancer (CRC) incidence in Lynch syndrome (LS) by detecting and removing adenomas. The existence of gene-specific differences in adenoma detection has been proposed yet remains insufficiently explored.
Carriers of MLH1/MSH2 pathogenic variants are at a higher risk of developing AAs compared with those with MSH6/PMS2 mutations, with MSH6 carriers exhibiting an intermediate risk profile. Advanced adenomas(AA) are an independent risk factor for post-colonoscopy CRC . LS patients with AAs should be identified as high risk and undergo enhanced colonoscopy surveillance.
https://www.sciencedirect.com/science/article/abs/pii/S001650852500650X?dgcid=author
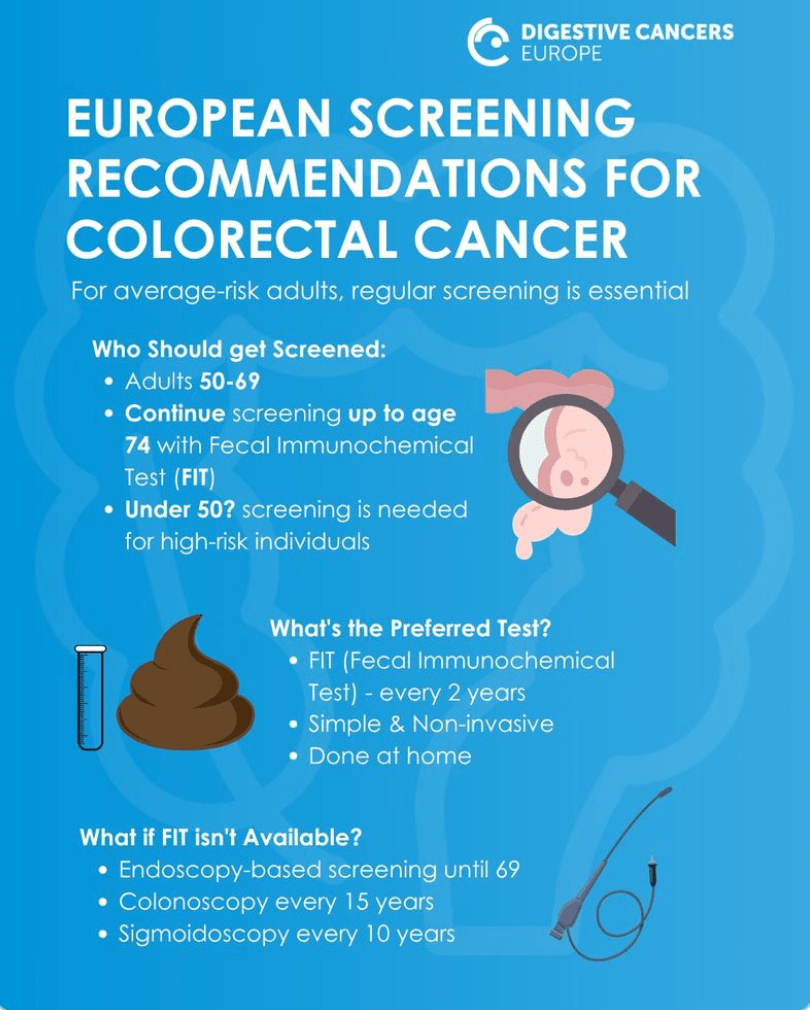
The European Commission’s Joint Research Centre (JRC) has just published updated recommendations on colorectal cancer screening tests and strategies for getting people to participate in screening.
Combining two immunotherapy drugs is a more effective treatment for certain metastatic colorectal cancers than using either treatment drug alone.
CheckMate 8HW trial used together, Opdivo (nivolumab) plus Yervoy (ipilimumab) slowed cancer growth in MSI-High metastatic colorectal cancers, a type of colorectal cancer often found in Lynch syndrome.
The FDA approved this combined treatment for MSI-High metastatic colorectal cancer after progression with chemotherapy.
Note: People with Lynch syndrome who have colorectal cancer commonly have MSI-H or dMMR cancers.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(24)02848-4/abstract
Please consider joining our closed group if you have inherited the Lynch syndrome predisposition to cancer or are part of a family that has this mutation. We would love to welcome you.
Simple process…just select the “Sign Up” button on our open Facebook page.
https://www.curetoday.com/view/iv-complications-and-the-challenge-of-being-heard