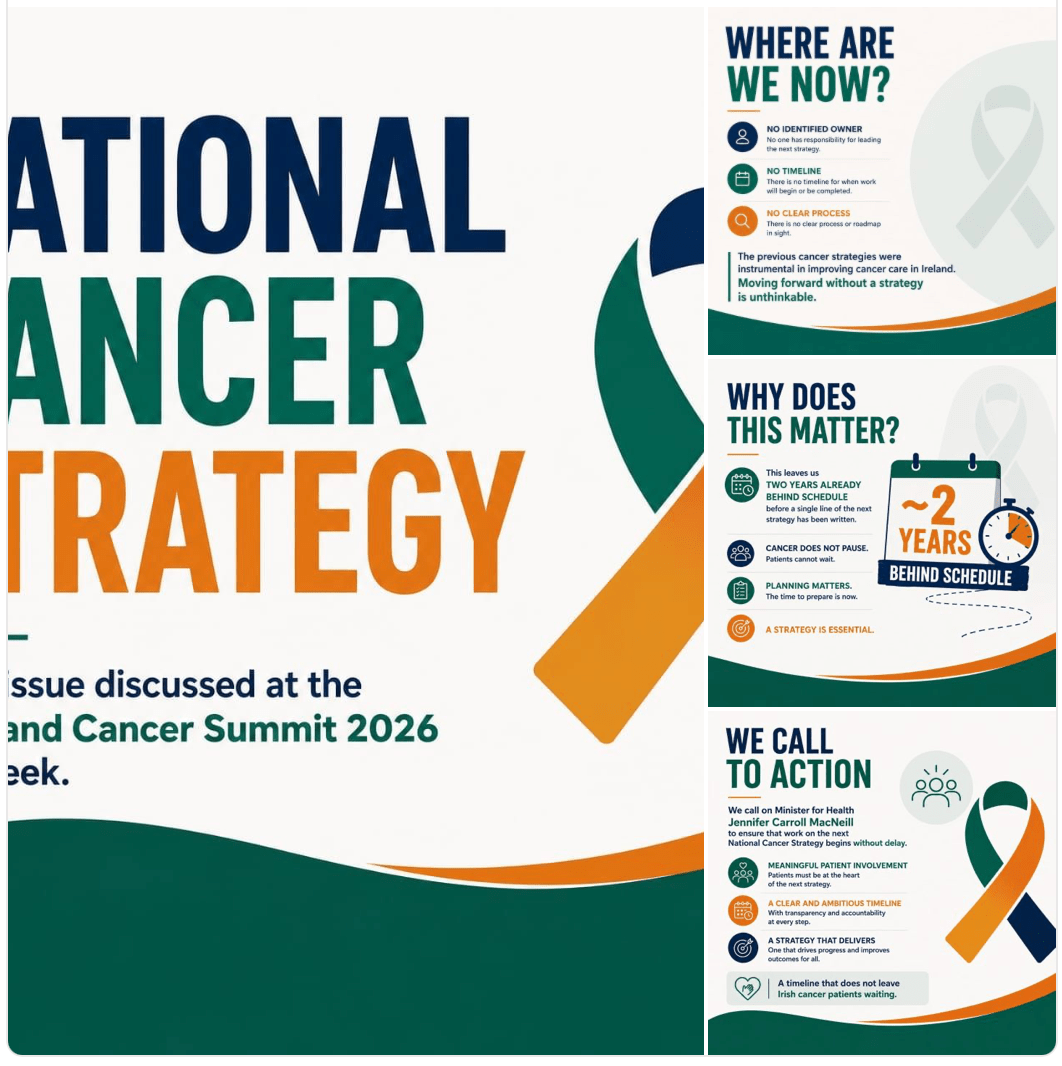
The launch of The Future of Advanced Cancer Therapies in Ireland white paper at the All-Island Cancer Summit shone a spotlight on a stark reality: Ireland is producing world-class cancer innovation, yet many patients still cannot access the latest treatments.
Challenges Identified
- Limited infrastructure and workforce capacity to deliver complex therapies.
- High costs associated with advanced treatments.
- Need for improved biomarker testing and precision medicine capabilities.
- Insufficient clinical trial capacity compared with leading international centres.
- Geographic and socioeconomic disparities in access to care.
Recommendations
- Accelerate patient access to innovative cancer medicines.
- Strengthen national infrastructure for advanced therapies.
- Expand specialist workforce training and recruitment.
- Increase investment in cancer research and clinical trials.
- Improve data collection and use of real-world evidence.
- Enhance collaboration across the island of Ireland to share expertise and resources.
- Develop long-term funding and policy frameworks to support adoption of breakthrough treatments.
My own thoughts on this are: We are great at producing reports and plans/white papers but very poor at looking at the waste within the Health System(too many administrators etc causing untold delays and waste) and ensuring that someone is responsible for delivery.
https://www.businesspost.ie/commercial-reports/the-next-wave-in-cancer-care