Menopause is an inevitable life stage for half the world’s population, but experiences vary hugely. Some women have few or no symptoms over the menopause transition while others have severe symptoms that impair their quality of life and may be persistent.
Many women feel unsupported as they transition menopause. To better prepare and support women, the Lancet Series on menopause argues for an approach that goes beyond specific treatments to empower women with high-quality information, tools to support decision making, empathic clinical care, and workplace adjustments as needed.
Prof Donal Brennan, Professor of Gynaecological Oncology in the UCD School of Medicine, University College Dublin, and colleagues have published a new featured review on menopause treatment for cancer patients.
Review aims to implement a more personalised and multidisciplinary approach in treatment of menopause symptoms after cancer.
(What about after surgical menopause?)
The article provides a comprehensive view of the current hormonal and non-hormonal therapy options studied and suggests a framework for more cost-effective and patient-focused models of care to meet the needs of a growing population of cancer survivors.
“Patients have repeatedly highlighted the burden of menopause symptoms after cancer treatment. They feel that these are often minimised or in some cases ignored,” said Prof Brennan. “
Key treatment advice points include:
MHT is an effective treatment for vasomotor symptoms and seems to be safe for many patients with cancer, the paper states.
Women younger than 45 years without contraindications should be offered an individualised treatment plan including MHT after cancer treatment.
If MHT is contraindicated, non-pharmacological and non-hormonal treatments are available for vasomotor symptoms; vaginal oestrogen seems to be safe for most patients with cancer and growing evidence supports safety after breast cancer.
Multidisciplinary management of menopause after cancer is essential and should include primary care and, if appropriate, allied health practitioners.
“As much as knowing more about your cancer can be debilitating, it can also be liberating. A well-informed patient can engage in substantive conversations with their doctors. It allowed me to participate in my care rather than having it done to me.”
Comprising over 9,000 patients with Lynch syndrome….Aims to improve the treatment of all patients living with the genetic condition.
Researchers from the Institute of Cancer Research (ICR), in collaboration with the National Disease Registration Service, the NHS Genomic Medicine Service Alliances and the NHS Regional Clinical Genetics Services, have set up the UK’s first-ever comprehensive database registry for Lynch syndrome patients to prevent cancer.
“By centralising patients’ genetic data, together with detailed information about the cancer diagnosis and treatments that these patients have received, researchers will gain crucial insights into Lynch syndrome… [unlocking] new opportunities for precision medicine and prevention, ultimately improving the lives of patients living with the condition.”
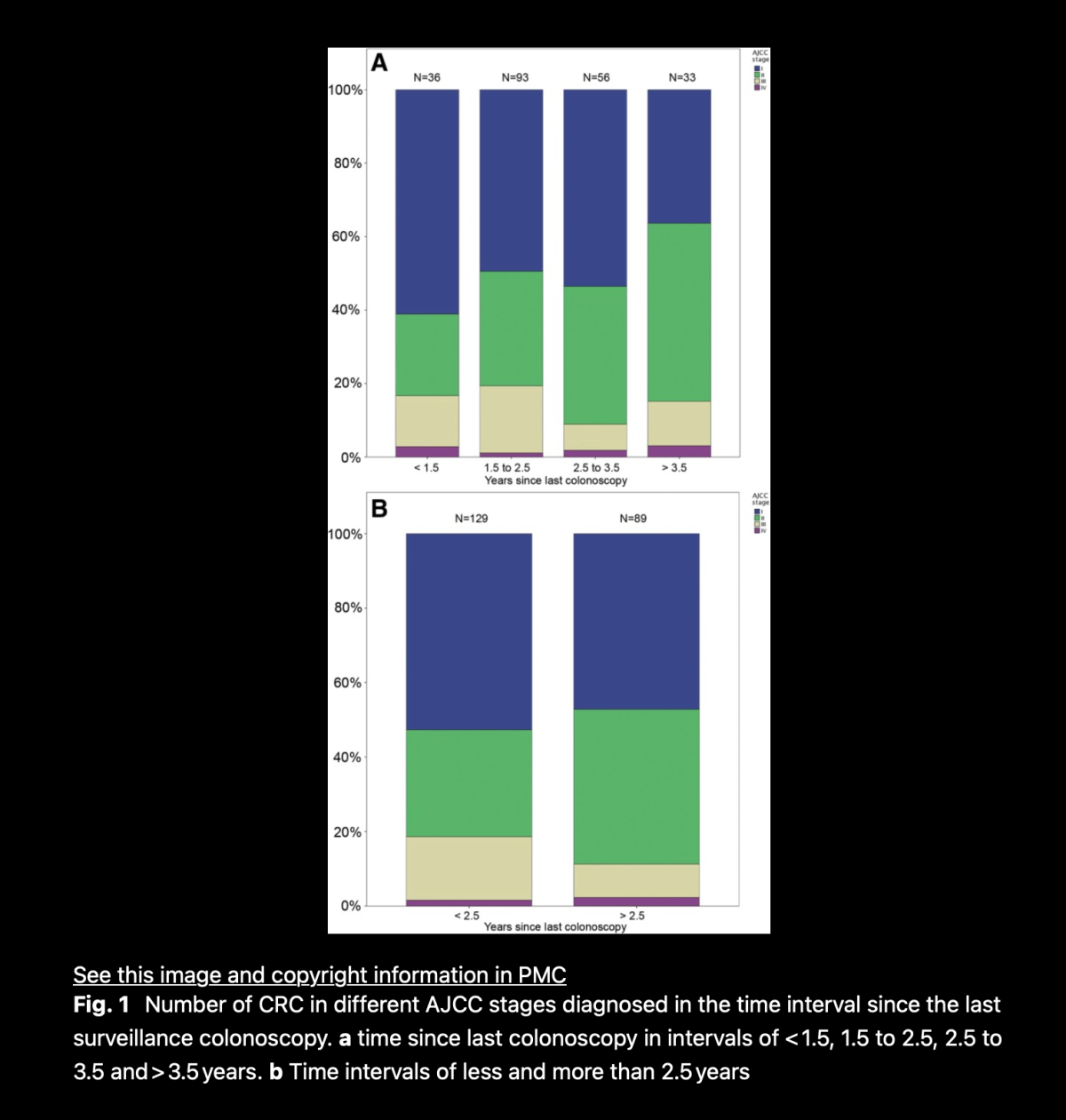
Recent epidemiological evidence shows that colorectal cancer (CRC) continues to occur in carriers of pathogenic mismatch repair (path_MMR) variants despite frequent colonoscopy surveillance in expert centres. This observation conflicts with the paradigm that removal of all visible polyps should prevent the vast majority of CRC in path_MMR carriers, provided the screening interval is sufficiently short and colonoscopic practice is optimal.
Our findingsraise the possibility that some CRCs in path_MMR carriers may spontaneously disappear: the host immune response may not only remove CRC precursor lesions in path_MMRcarriers, but may remove infiltrating cancers as well. If confirmed, our suggested interpretation will have a bearing on surveillance policy for path_MMR carriers.
Individual barriers such as feelings of fear, guilt, and anxiety and limited knowledge about Lynch syndrome as well as interpersonal barriers including complex family dynamics and language barriers limit family communication about Lynch syndrome and prevent uptake of genetic screening for relatives.
Organisational and environmental barriers including a shortage of genetics professionals, high costs, and fears of discrimination also reduce cascade testing.
These multi-level barriers may disproportionately impact underserved populations in the United States, such as individuals with lower incomes, limited English-speaking proficiency, lower educational attainment, and inadequate access to health systems.
As much as I want to believe my doctors are beyond brilliant and can do anything, they are people too. Much like me, they have good days and not-so-great ones.
What are the signs your doctor isn’t listening?
Constant interruptions.
Fidgeting.
There but not there.
Aggressive body language.
I make sure my doctor is listening by:
Being prepared.
Being courteous.
Rewinding the conversation.
As a last step, change doctors.
Rather than shrink back from having a “tough” conversation with a doctor, it is critical to do just that. Often these types of conversations, rather than ending a relationship with a doctor, strengthen it.
Scanxietyis a term coined to describe the mix of fear, anxiety and stress associated with medical scans.
The anticipation of undergoing medical procedures only adds another layer of stress. The anxiety and discomfort during scans heighten my sense of vulnerability and helplessness. As someone who has witnessed the toll of cancer on my brothers, the death of my eldest brother firsthand triggers traumatic memories, intensifying the emotional turmoil.
By acknowledging and addressing my emotional needs, I’m learning to navigate the rollercoaster of anxiety with resilience and grace and looking forward to brighter days ahead.
The advances in vaccine technologies,such as in Lynch Syndrome, is a promising field of research that has the potential to reduce the risk of developing cancer, thereby preventing disease and modifying surveillance regimens for high-risk patients.
What To Do While We Wait for a Vaccine
While the possibility of a Lynch Syndrome vaccine certainly brings a lot of hope and anticipation, it’s important to continue other preventative measures in the meantime. It is recommended that Lynch Syndrome patients:
Receive regular cancer screenings as advised by their healthcare providers.