
Clodagh Downing was experiencing symptoms for at least two years before her diagnosis of colorectal cancer, including recurring infections, an allergy to dairy, irregular bowel movements and bloating. Her blood tests were clear but when she developed fatigue and anaemia, a Google search suggested bowel cancer. In January 2021, she asked her GP for a colonoscopy. But at 48, her doctor told her she was too young.
Author: Lynch Syndrome Ireland
Talking with Children About Adult-Onset Hereditary Cancer Risk:

Often complicated by the parent’s ongoing adjustment to their mutation status, guilt at potential transmission of the mutation to the child, concern over inciting distress in children, and the varied capacities of children in the home to understand genetic information.
Optimally, communication about inherited cancer risk is an open, ongoing process within the family.
Early-Onset GI Cancers: Rising Trends, Genetic Risks, Novel Strategies, and Special Considerations
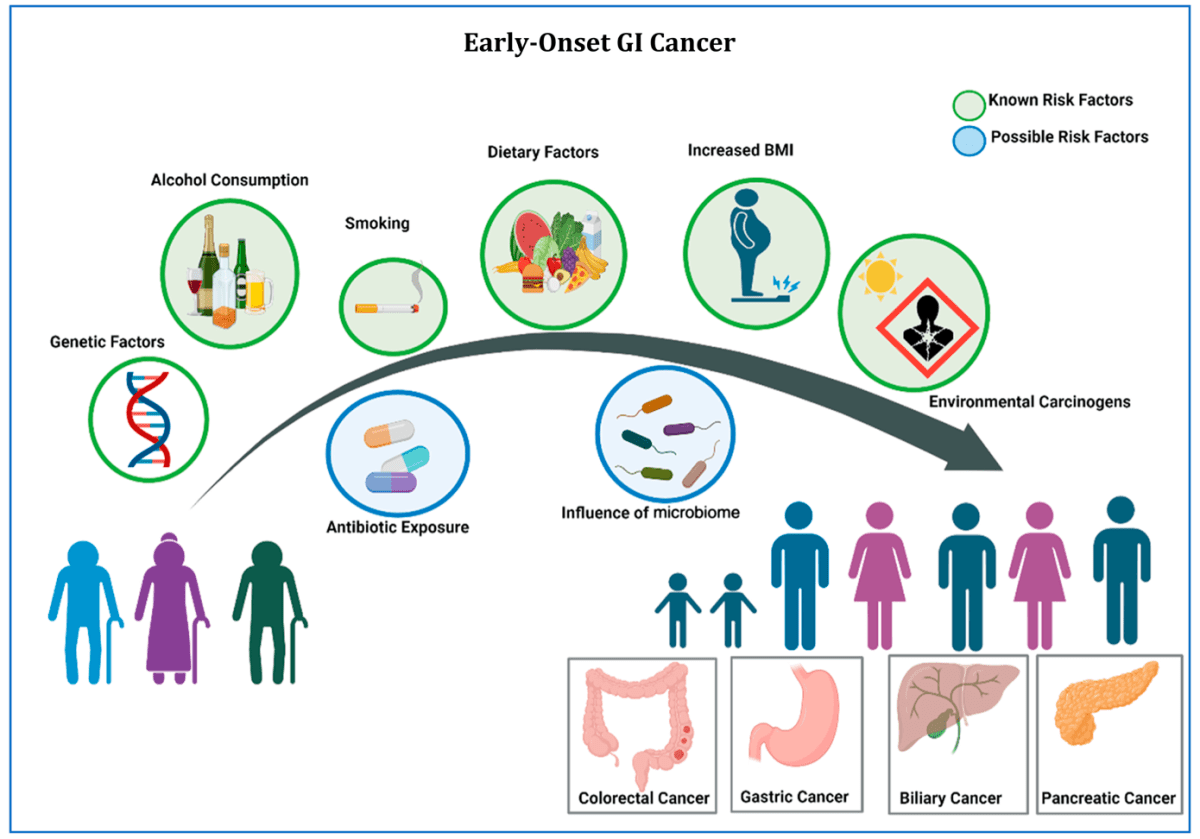
Understanding the complex interplay between host factors such as gPVs (Germline Pathogenic Variant), gut microbiome, and extrinsic environmental factors will be critical to mitigate the rising incidence of EO cancer globally, particularly across the spectrum of GI cancers.
Practical Applications
Awareness of the early-onset (EO) cancer epidemic should prompt heightened vigilance among health care providers caring for patients who would not be historically considered at high risk for cancer.
Early detection of symptoms with appropriate diagnostic testing is critical to obtaining a cancer diagnosis in earlier stages which may allow for a greater chance of curative approaches.
Multidisciplinary management of patients with EO cancers is critical to address unique and challenging issues that younger populations must navigate, including family, social, career, and financial stress.
Genetic counselling and testing are critical components to multidisciplinary care and may elucidate mechanisms of EO cancer development.
Study Finds New Role For Vitamin D In Cancer Treatment
“These results suggest that vitamin D supplementation in patients with lower levels of vitamin D may reduce peripheral neuropathy, and particularly high-grade peripheral neuropathy, which would improve these patients’ long-term quality of life,” said senior researcher Daniel L. Hertz, PharmD, PhD, of the University of Michigan College of Pharmacy.
Remembering My Brother Who Died of Cancer
Survivor guilt is a complex emotion that often plagues those who have lost loved ones to illness.
I question myself with overwhelming questions often: “Why have I not developed cancer? Why have I outlived him? Why did he have to die?” And “What could we as a family have done differently?
I have turned my grief into action and strive to make a positive impact in the fight against Lynch syndrome and its devastating consequences — his death has not been in vain.
https://www.curetoday.com/view/remembering-my-brother-who-died-of-cancer
Landmark national study supports use of whole genome sequencing in standard cancer care(UK)

In the largest study of its kind, scientists today report how combining health data with whole genome sequence (WGS) data in patients with cancer can help doctors provide more tailored care for their patients.
This research uncovered significant findings across different cancer types, such as:
- Over 90% of brain tumours and over 50% of colon and lung cancers showed genetic changes that could affect how patients are treated, guiding decisions about surgery or specific treatments they might need.
- In more than 10% of sarcomas, larger DNA changes, known as structural variants, were identified that can impact clinical care and treatment.
- In over 10% of ovarian cancers, the study pinpointed inherited risks offering crucial insights for clinical care.
The findings show the value of combining genomic and clinical data at scale to help healthcare professionals make the best treatment decisions with their patients.
Hereditary Cancer Rounds – Describing the Real World Experience of Implementing a Pre-test GC Portal
Had similar issues to Ireland…long waiting list for Genetic Counselling etc. Using technology they have improved their situation.
The Hereditary Cancer Program provides genetic counselling and genetic testing for BC/Yukon residents who may have inherited an increased risk for certain types of cancer.
An interactive animation about LynchSyndrome
Patient-facing genetic and genomic mobile apps in the UK: a systematic review of content, functionality, and quality(2022)
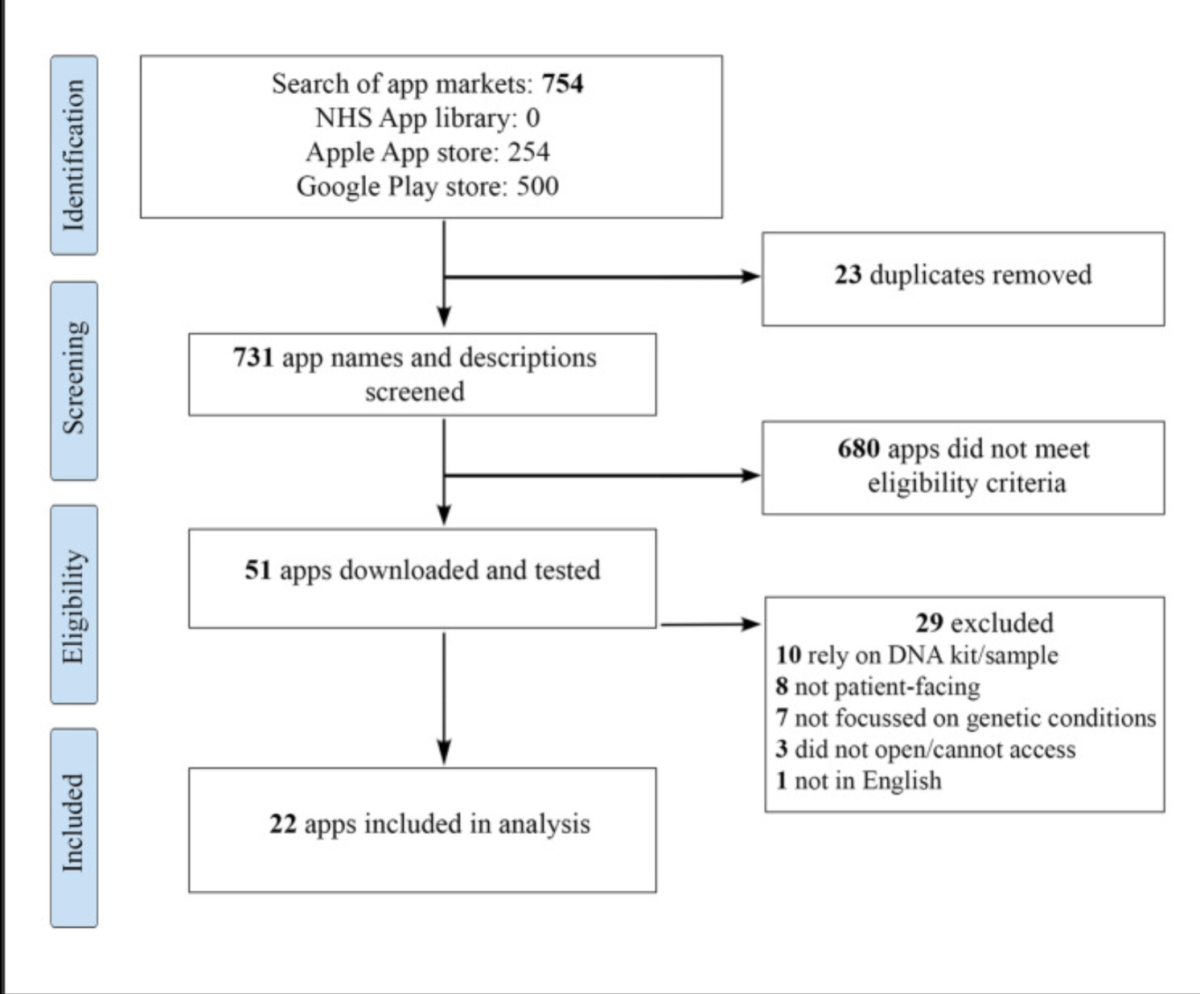
This systematic review of patient-facing genetic/genomic mobile apps explores content, function, and quality.
Conclusion: It was evident that there are few high-quality genomic/genetic patient-facing apps available in the UK. This demonstrates a need for an accessible, culturally sensitive, evidence-based app to improve genetic literacy within patient populations and specific communities.
Has this changed?
Study: Immunotherapy improves outcomes of advanced endometrial cancer

Standard treatment for advanced endometrial cancer may soon change. A study found that people with advanced or recurrent endometrial cancer who received immunotherapy with chemotherapy had better outcomes than those who had chemotherapy alone.
https://www.facingourrisk.org/XRAY/immunotherapy-improves-advanced-endometrial-cancer-outcomes
