Knowing your family history of cancer is a critical aspect of cancer prevention and early detection.
Many types of cancer, including Lynch syndrome-related cancers, have a hereditary component. This means that individuals with a family history of cancer may be at increased risk for developing the same or related types of cancer.
The more you know about your family’s cancer history, the better equipped you will be to make informed decisions about your own health and to take proactive steps to reduce your risk of cancer.
Lynch syndrome may affect up to 175,000 people in the UK and is linked to 3% of cases of womb cancer. To develop Lynch syndrome, you need to have one parent that carries the gene. Someone diagnosed with Lynch syndrome has up to 60% chance of developing womb cancer in their lifetime. Lynch syndrome is also associated with an increased risk of bowel cancer. Those diagnosed with Lynch syndrome undergo regular tests to check for bowel cancer and womb cancer, many will be offered a hysterectomy (operation to remove the womb) to prevent womb cancer once they feel their family is complete.
Lynch syndrome is often diagnosed when a strong family history of bowel or womb cancer is noted. If you feel this may apply to you, please speak to your doctor about being referred to a genetics service. More information on Lynch syndrome can be found here.
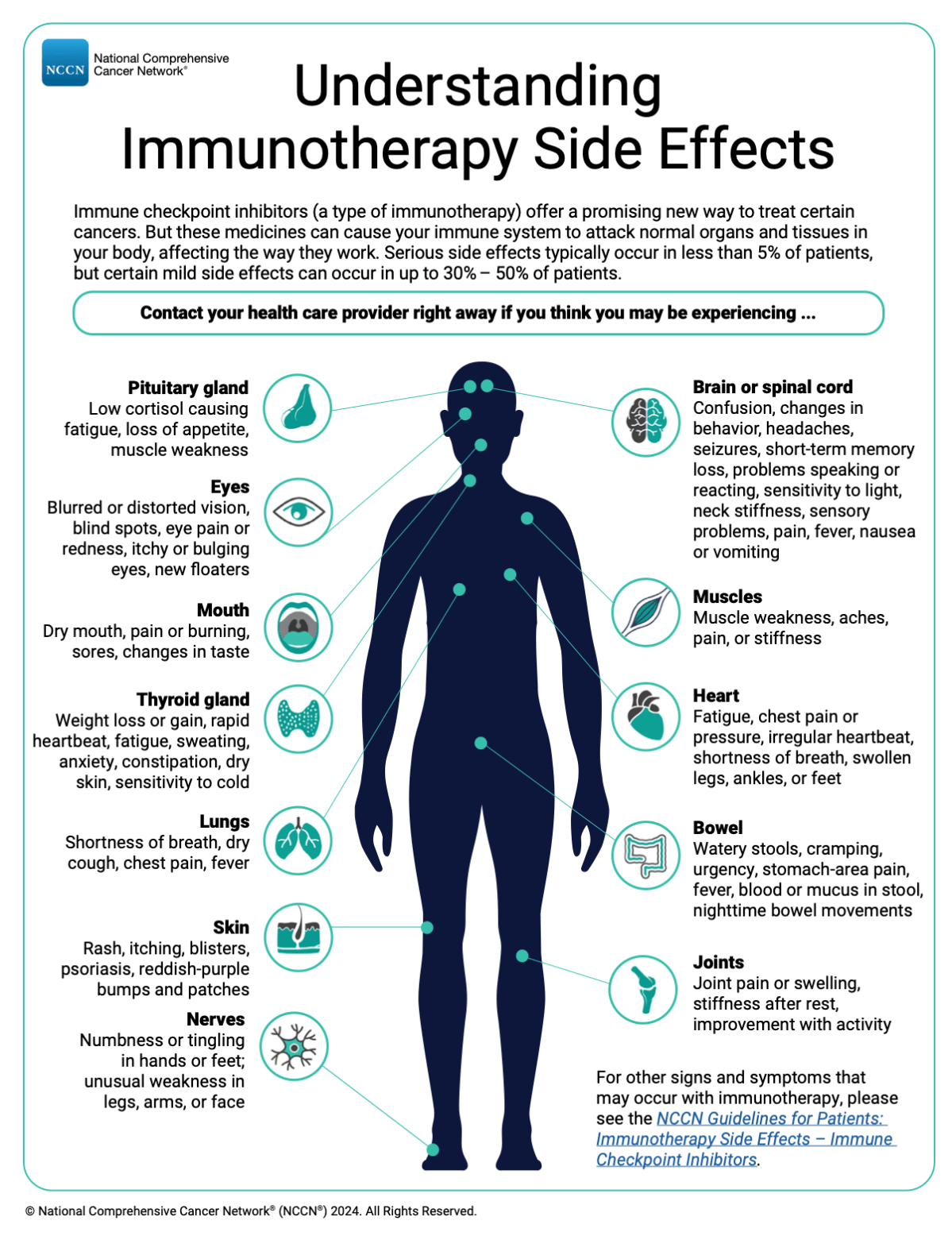
Immune checkpoint inhibitors (a type of immunotherapy) offer a promising new way to treat cancer for some patients. But these medicines can cause your immune system to attack normal organs and tissues in your body, affecting the way they work.
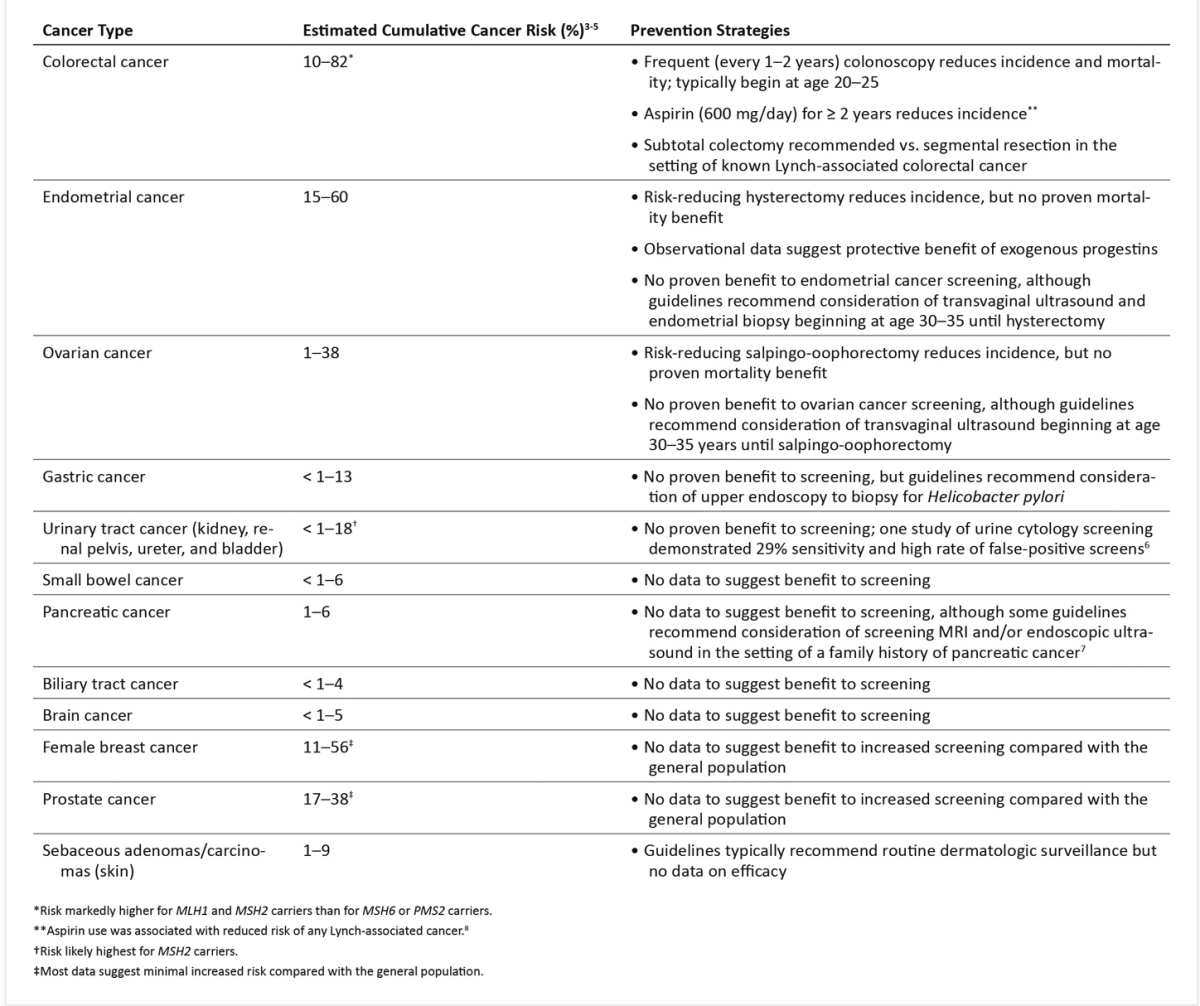
For women with Lynch syndrome, endometrial cancer and ovarian cancer represent the second- and third-most common associated malignancy, respectively, after colorectal cancer.
Despite gaps in knowledge, most guidelines currently recommend consideration of risk-reducing hysterectomy and salpingo-oophorectomy at the completion of childbearing and/or in the early 40s, with consideration of annual transvaginal ultrasound and endometrial biopsy at age 30 to 35 (continued until risk-reducing surgery).
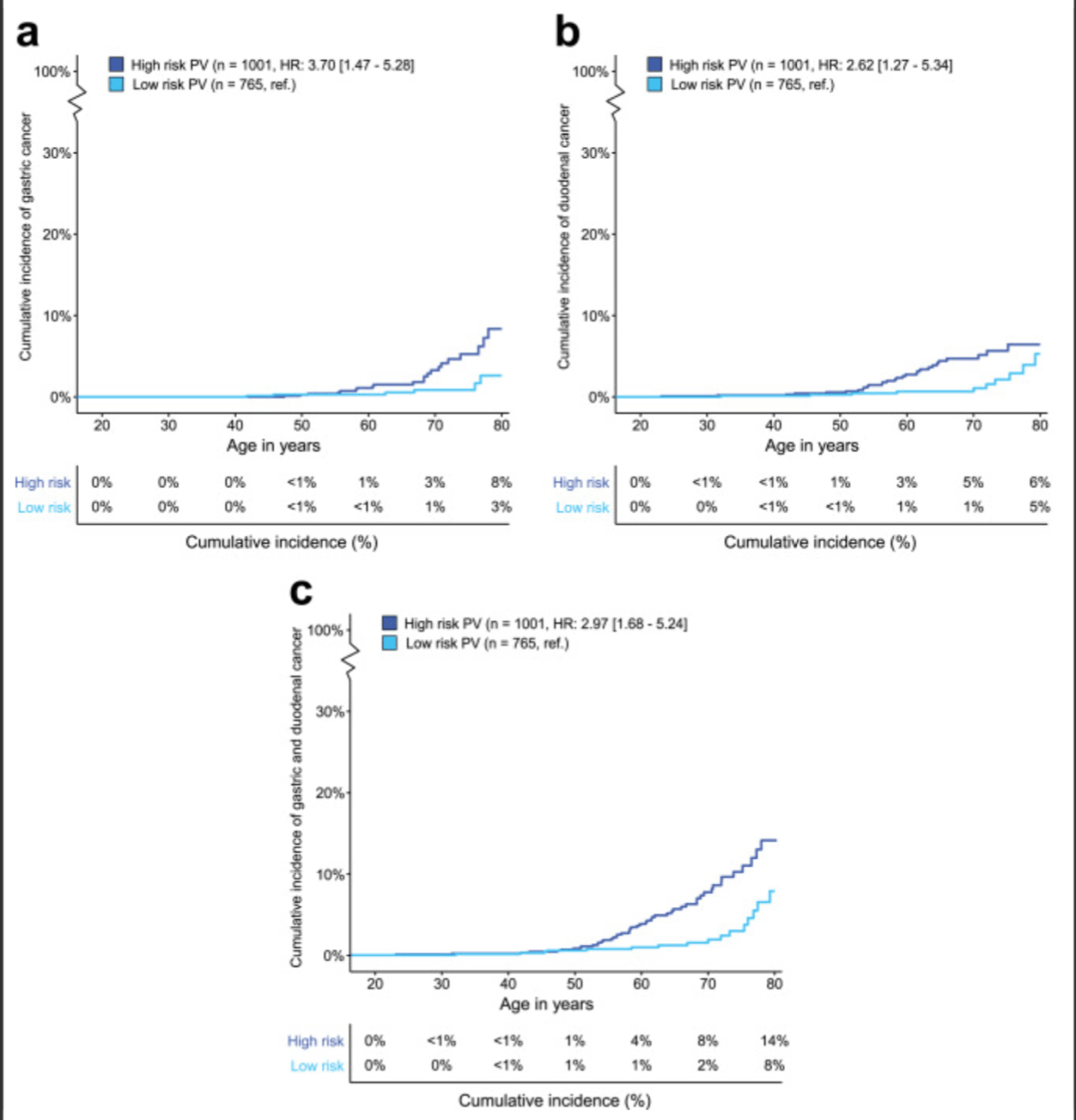
The benefit of EGD surveillance in individuals with Lynch syndrome is still a topic of debate.
Considering the invasive nature of the procedure, the patients’ burden, and—albeit small–the risks associated with conscious sedation and the procedure itself, it is essential to provide EGD surveillance only to individuals at high risk of developing GC and DC who could benefit from this procedure.
Researchers have linked abnormal DNA methylation to several adverse outcomes, including human diseases.
So far, much of this research has been focused on cancer and tumour suppressor genes, since hypermethylation often results in the silencing of tumour suppressor genes in cancerous cells.
Compared to normal cells, the genomes in cancer cells have also been shown to be hypomethylated over all, with hypermethylation only occurring in the genes involved in tumour cell invasion, cell cycle control, DNA repair and other processes where silencing would lead to the spread of cancer.
In colon cancer, it is possible to detect hypermethylation early on in the course of disease, meaning hypermethylation may serve as a biomarker for the condition.
The decision regarding the multiple approaches to rectal cancer can be very challenging:
Summary
The NCCN Rectal Cancer Panel believes that a multidisciplinary approach, including representation from gastroenterology, medical oncology, surgical oncology/colorectal surgery, radiation oncology, pathology, and radiology, is necessary for treating patients with rectal cancer.
Patients with very-early-stage tumours that are T1, N0 and who meet carefully defined criteria can be managed with ESD or transanal local excision. A transabdominal resection is appropriate for other rectal lesions. A TNT approach, traditionally consisting of chemoRT/short-course RT and chemotherapy, is preferred when RT is being given.
However, ongoing clinical trials for rectal cancer are particularly focused on treatment approaches that omit surgery or RT, with the goal of improving outcomes for eligible patients. Careful surveillance is necessary to detect and manage recurrences in a prompt and effective manner.