Category: Screening
Mortality by age, gene and gender in carriers of pathogenic mismatch repair gene variants receiving surveillance for early cancer diagnosis and treatment: a report from the prospective Lynch syndrome database

The current study found low CRC mortality in path_MMR carriers who receive colonoscopy surveillance while some extracolonic cancers were associated with high mortality. Further improvement of survival in LS may require a focus on the prevention and treatment of non-colorectal cancers, likely including approaches based upon the immune response to MSI pre-cancerous lesions and cancers.
This study also provides more precise cumulative cancer incidences for path_MMR carriers than have been available previously, stratified by age, gene, organ, and gender.
https://www.sciencedirect.com/science/article/pii/S258953702300086X
What is Lynch Syndrome?

Be aware of gene changes and cancer in your family and take part in screening to reduce your risk of cancer.
Early-Onset Colorectal Cancer (EOCRC)
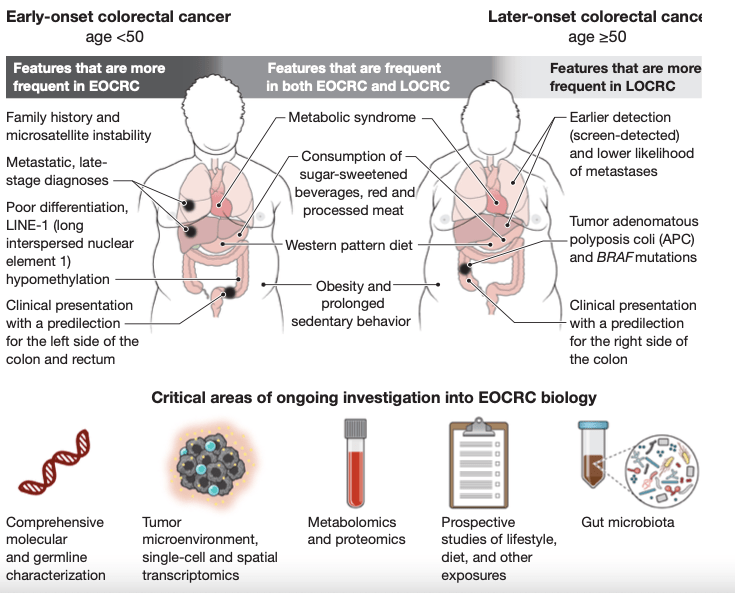
Patients with EOCRC have a higher relative prevalence of inherited predisposition to cancer, with Lynch syndrome being the most common cause.
Colorectal cancer in younger people
Similar factors increase the risk of early-onset colorectal cancer (EOCRC) and later-onset colorectal cancer (LOCRC), such as a sedentary lifestyle, obesity, and metabolic syndrome, but there are also important differences. EOCRC predominantly occurs on the left side of the colon and the rectum, whereas LOCRC arises more commonly on the right side of the colon. EOCRC is also more poorly differentiated and often metastatic at diagnosis.
Research is urgently needed to understand the increasing incidence of EOCRC and its pathophysiology to better detect and treat patients.
Constitutional (germline) vs Somatic (tumour) variants

Constitutional (also known as germline) variants are present in all the body’s cells, including the germ cells, and can therefore be passed on to offspring; somatic variants arise during an individual’s lifetime in tissues other than the germ cells and so are not passed on.
The identification of a germline variant in a mismatch repair (MMR) gene in a patient with colorectal cancer has implications for the clinical management of the current cancer and the patient’s future cancer risk. It should also trigger cascade screening in the wider family.
(Cascade testing is the process of informing family members of a genetic condition discovered within the family, followed by family members getting tested for the condition.)
Lynch syndrome prediction model

The PREMM5 model is a clinical prediction algorithm that estimates the cumulative probability of an individual carrying a germline mutation in the MLH1, MSH2, MSH6, PMS2, or EPCAM genes. Mutations in these genes cause Lynch syndrome, an inherited cancer predisposition syndrome.
N.B.:This website is provided for informational purposes only. The content is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your doctor or other qualified health provider with any questions you may have regarding your personal health or medical condition.
Lynch Syndrome
Lynch Syndrome
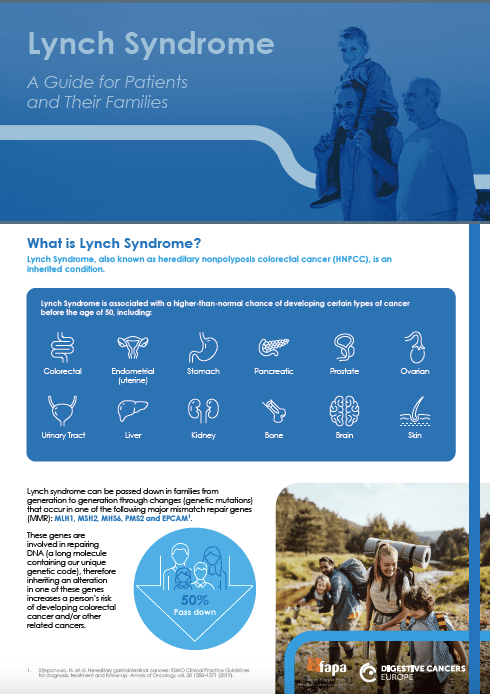
A Guide for Patients and Their Families
Lynch Syndrome is associated with a higher-than-normal chance of developing certain types of cancer before the age of 50.
What does it mean to live with Lynch Syndrome?
Delphi Initiative for Early-Onset Colorectal Cancer (DIRECt) International Management Guidelines
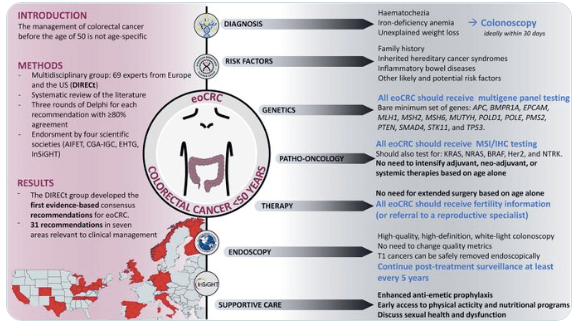
Conclusions
The DIRECt group produced the first consensus recommendations on eoCRC. All statements should be considered together with the accompanying comments and literature reviews. We highlighted areas where research should be prioritized. These guidelines represent a useful tool for clinicians caring for patients with eoCRC.
Results
The DIRECt consensus produced 31 recommendations for patients diagnosed with eoCRC ≥18 years old based on 145 articles (summarized in Supplementary Appendices 2–7). When appropriate, issues related to colon or rectal cancers specifically are highlighted; in cases where statements applied to both colon and rectal cancer, the term colorectal cancer (CRC) was used.
All statements are summarized in Table 2, Table 3, Table 4(Table 2: diagnosis, risk factors, and genetics; Table 3: pathology, oncology; Table 4: endoscopic diagnosis and treatment, therapy, and supportive care). Areas of controversy are described throughout the main text and summarized in Table 5.
Roberta
I’ve been given the gift of information,while it can be physically & emotionally taxing, I can take steps to ensure colorectal cancer doesn’t end my life.I can help others have the courage to get tested & go for screening if they notice a change.
When asked what she wanted people to take away from her contribution to the Marie Keating Foundation’s #JoinTheBowelMovement campaign this April, Roberta’s message was simple.
“Firstly, get to know your family history and the signs and symptoms of bowel cancer. Secondly, if you are experiencing symptoms but don’t fit the idea in your mind of “what a bowel cancer patient is”, speak to your GP about it anyway. And finally, if you’re eligible, go for BowelScreen. It’s so much easier to prevent than to cure, so if you were to take something away from my story, I would want it to be that.”
