
Conclusion: Our qualitative findings demonstrate patients with CRC have a strong desire for healthcare systems to regularly implement and offer UTS.
Blog
Patience…A form of Action?

Can learning patience actually be an active effort? A 3 minute Side Trip with some reflection on my(Pat Wetzel) personal path to learning patience.
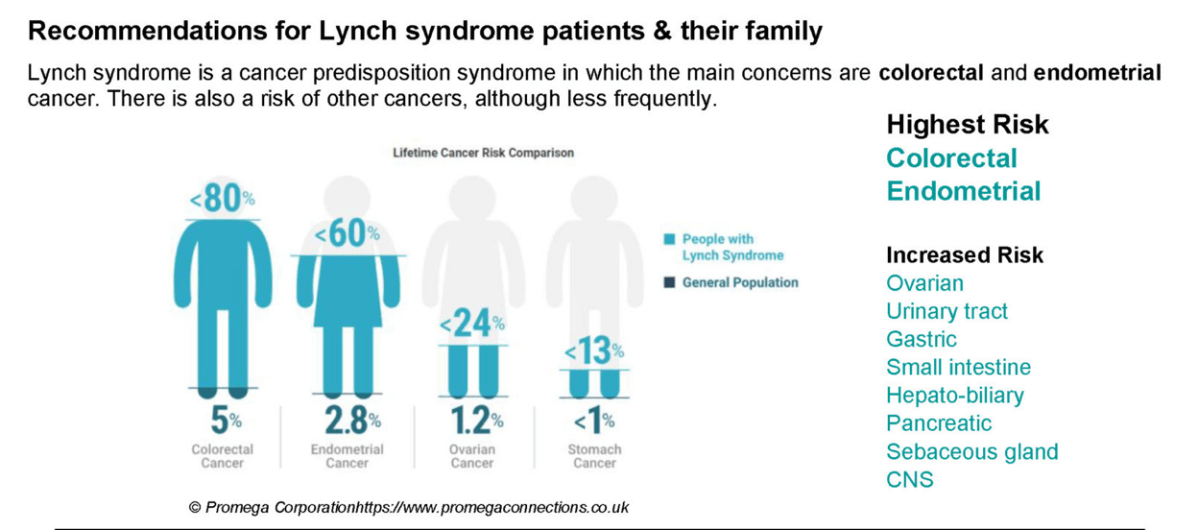
What is Lynch syndrome?
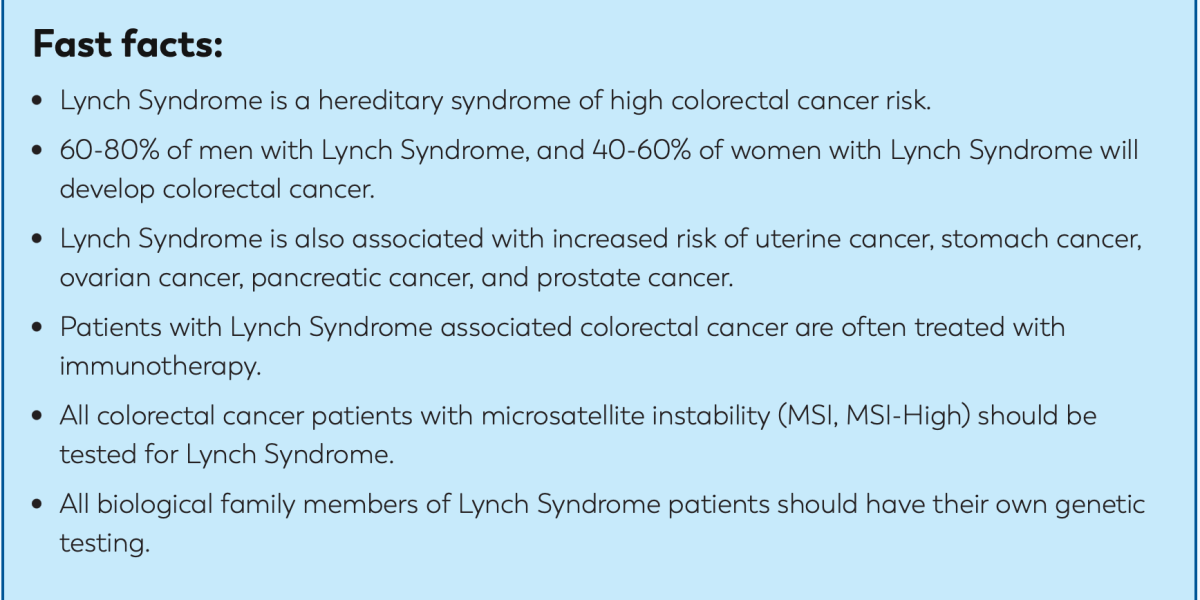
Talking about Lynch Syndrome: Strategies for discussing with your children and family
Screening for Lynch Syndrome in people aged 18-40 using a saliva test

A new Australian study published in The Lancet suggests population-wide genetic screening for hereditary breast and ovarian cancer, familial hypercholesterolemia and Lynch syndrome, in people aged 18 to 40, would be cost effective and save lives.
Modelling demonstrates a marked improvement in the overall cost-effectiveness of offering population genomic screening in a combined fashion for multiple conditions together, versus criteria-based clinical genetic testing or screening for individual conditions.
The model structure can be applied to other healthcare systems, making our findings relevant for international jurisdictions, especially countries with national public healthcare systems capable of delivering nation-wide population screening programs.
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(23)00474-1/fulltext
Lynch syndrome quick guide for Primary Care clinicians(NHS)
The training involves watching a short video which covers:
- A brief overview of Lynch syndrome
- Their personalised cancer prevention programme
- An introduction to the Lynch syndrome quick guide and how it can help you identify and manage your patient’s care
- How to manage their first-degree family members’ care
ColoMARK Project!
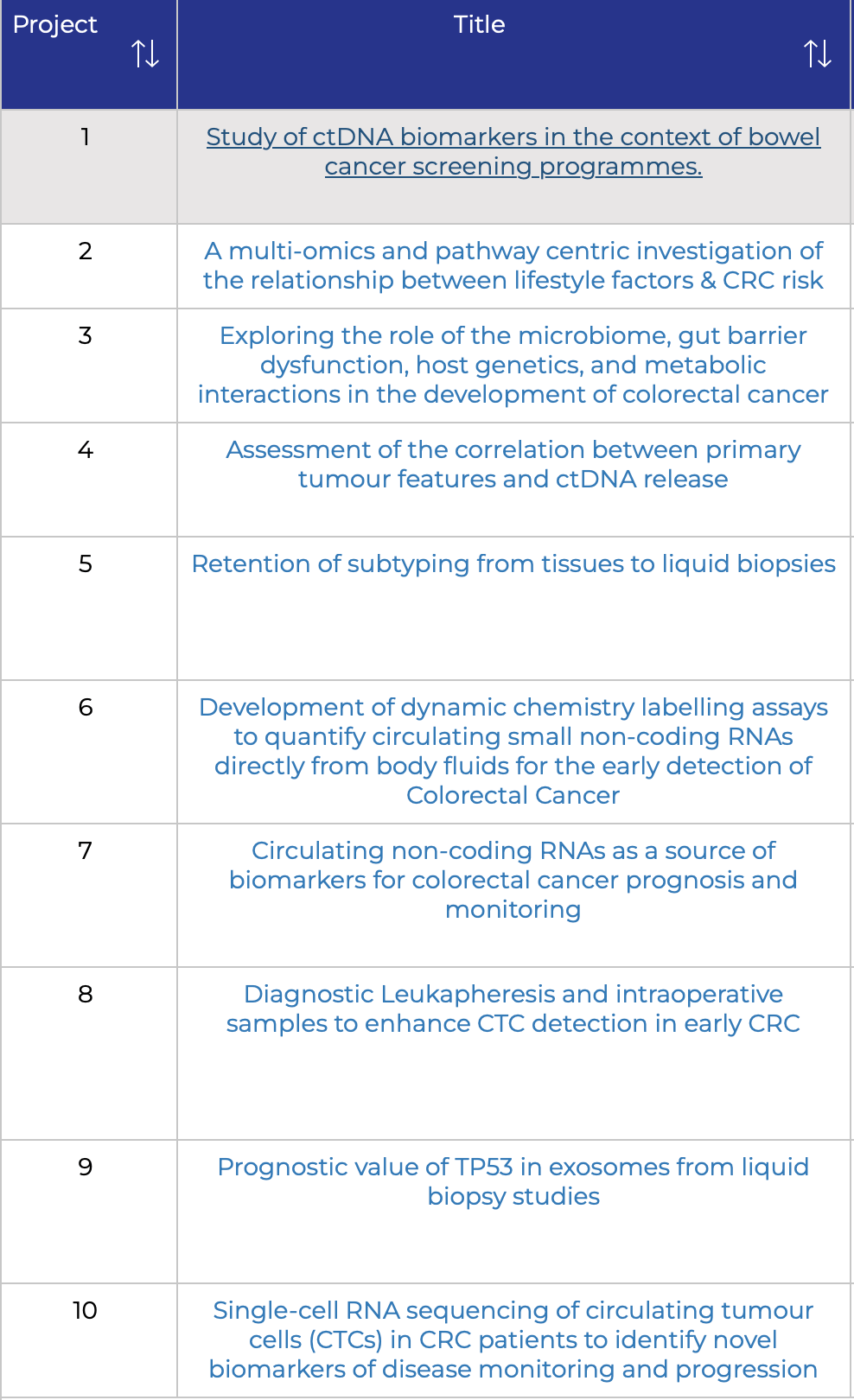
Identification and development of novel colorectal cancer biomarkers via state-of-the-art liquid biopsy approaches.
The primary scientific objective of ColoMARK will be to generate improved biomarkers for CRC by employing innovative liquid biopsy approaches. The impact of this project is paramount, as it will play a crucial role in advancing CRC prevention, treatment and management.
This project has received funding from the European Union’s Horizon Europe research and innovation programme under the Marie Sklodwska-Curie Doctoral Network Grant.
ctDNA has been widely evaluated as a novel biomarker for liquid biopsy in colorectal cancer diagnosis, prognosis and monitoring of response to treatment. Liquid biopsy based on ctDNA detection is a very sensitive test.
So how would I like to change healthcare? Part 3 of 3

Doctor, please……GetPersonal with me!
So how would I like to change healthcare? Part 2 of 3

- Every patient should be given easily understandable information about all aspects of their diagnosis
- Every patient should be told about all their options for treatment and care
- A patient should take responsibility for their lives and their diagnosis and work with the doctor
- Patients should not have to fight to get correct treatment
So how would I like to change healthcare? Part 1 of 3

I would like to see a dedicated organisation, with patients involved, looking at excellence in treatment
- This would not be an ever changing government looking at their own interests or survival.
- I would like to see centres of excellence, not general hospitals telling you, ‘There is no chance’
- I would like to see patients as the focus of their treatment, NOT their symptoms!
