Category: Uncategorized
Individual Health Identifier (IHI)

Did you know….
The Health Identifiers Act 2014 was enacted by the government to allow two new national data collections–called the National Register of Individual Health Identifiers and the National Register of Health Service Provider Identifiers to be created and operated.
An Individual Health Identifier (IHI) has the following benefits for you:
Improved accuracy in identifying you and your medical records will
lead to safer and better care being provided to you.
Improved accuracy in identifying and associating your records in
different healthcare organisations.
Your health information can be shared safely and seamlessly
between health service providers, for example on referral letters
sent from a private GP to a public hospital.
The use of an Individual Health identifier also enables the
electronic transfer of your health information, which results in faster
care for you.
Medical or clinical information will NEVER be stored on your IHI record. Health
service providers may however use your IHI, to uniquely identify you, when
communicating with other health service providers about your care for example
when a medical consultant is corresponding with your GP or visa versa.
Incidences of colorectal adenomas and cancers under colonoscopy surveillance suggest an accelerated “Big Bang” pathway to CRC in three of the four Lynch syndromes
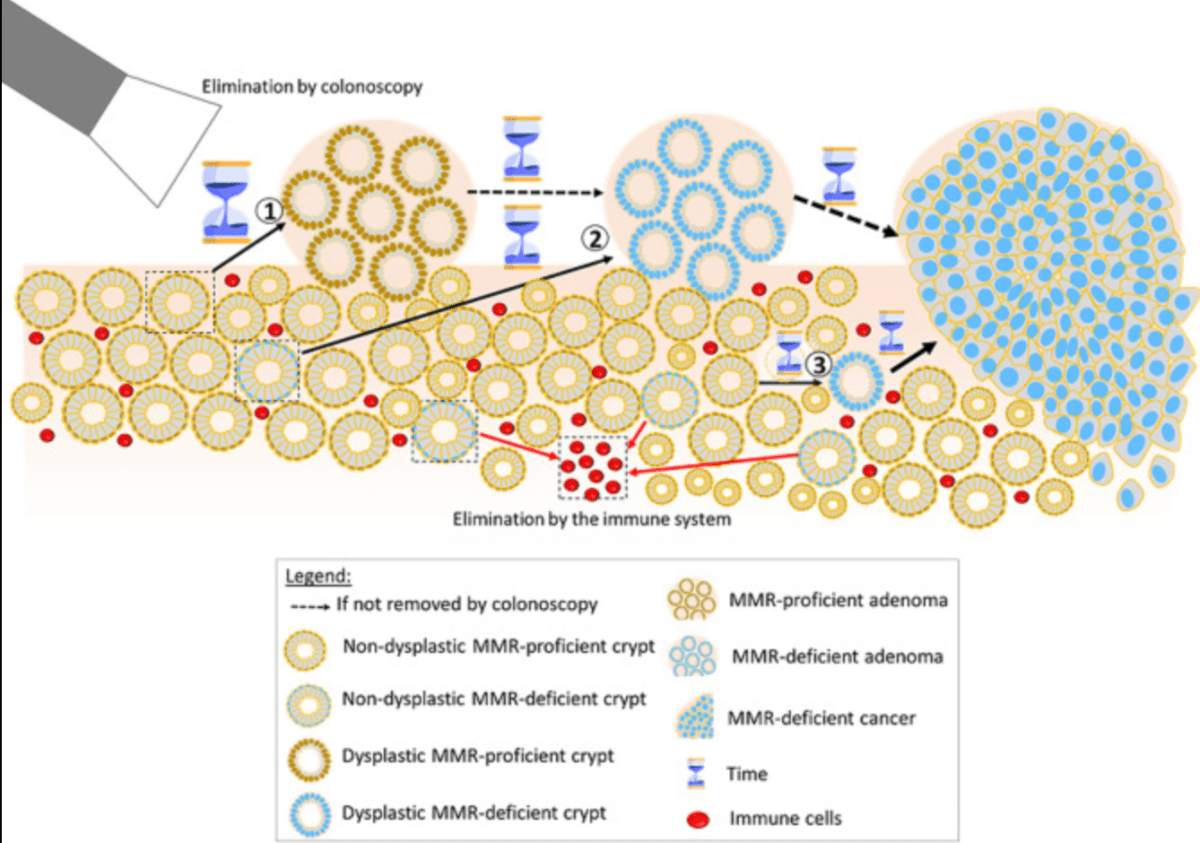
Conclusions: Colonoscopy prevented CRC in path_PMS2 carriers but not in the others. Our findings are consistent with colonoscopy surveillance blocking the adenoma-carcinoma pathway by removing identified adenomas which might otherwise become CRCs. However, in the other carriers most CRCs likely arised from dMMR cells in the crypts that have an increased mutation rate with increased stochastic chaotic probabilities for mutations. Therefore, this mechanism, that may be associated with no or only a short sojourn time of MSI tumours as adenomas, could explain the findings in our previous and current reports.
path_MMR:Pathogenic or likely pathogenic variant in one of the MMR genes (MLH1, MSH2, MSH6, or PMS2)
https://pubmed.ncbi.nlm.nih.gov/38741120/
Overall….colonoscopy works either by preventing some cancer, or where this is not biologically possible- by diagnosing cancer early.
[GDPR] is being used in Ireland as a reason not to do things, as an excuse not to share data
Where do non-invasive colorectal cancer tools ‘FIT’ alongside colonoscopy in the surveillance of high-risk patients?
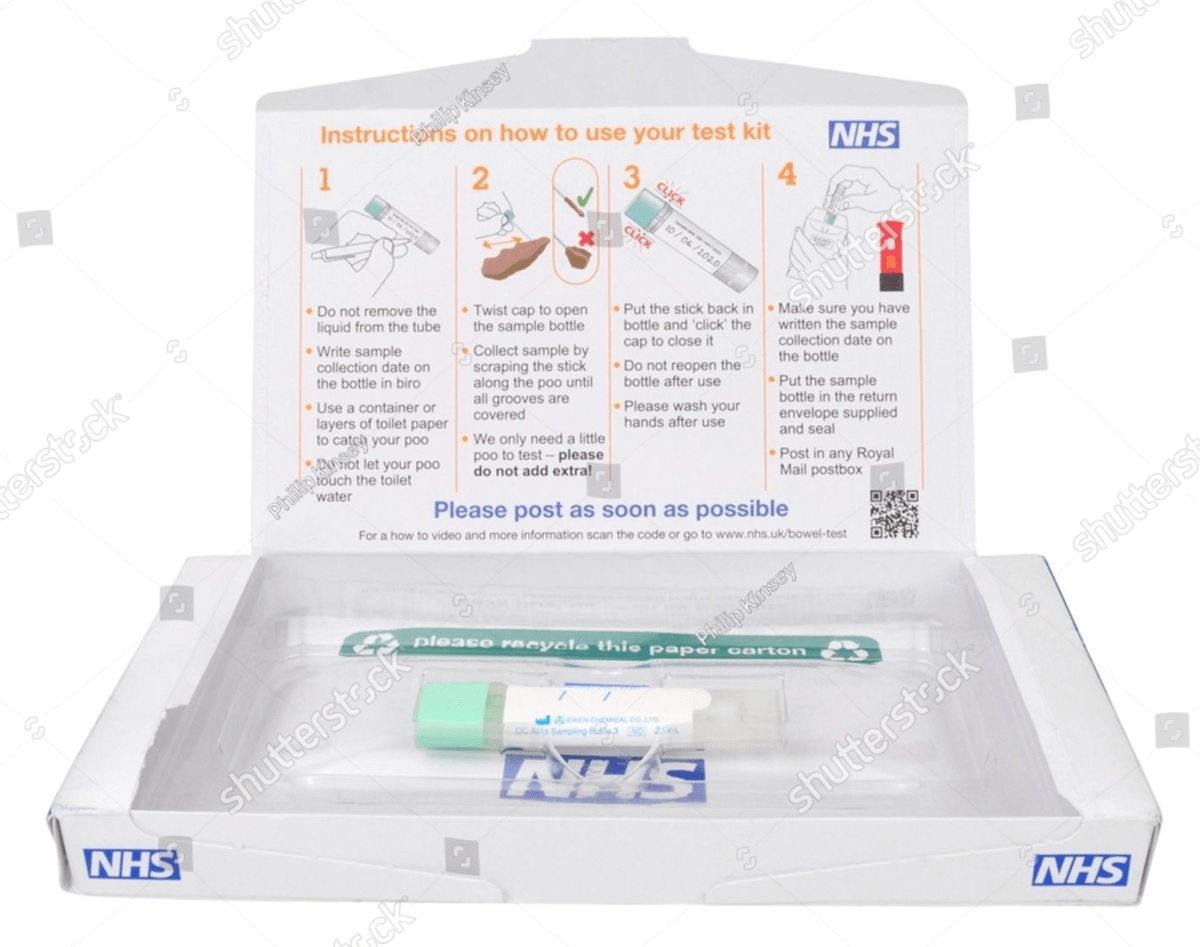
There is increasing interest in the use of less-invasive approaches to investigation of at-risk populations, driven in part by the COVID19 pandemic as resources have been increasingly constrained, alongside expanding evidence of clinical effectiveness.
Fecal hemaglobin immunochemical testing(FIT) has been validated in screening and symptomatic populations, is cost-effective, and acceptable to patients.
As a quantitative assay, lower fHb concentration thresholds increase CRC sensitivity albeit with decreased specificity, however FIT has a lower sensitivity for advanced adenomas of around 40-60%2. Therefore a ‘FIT only’ strategy may theoretically result in fewer prevented CRCs, notwithstanding a limited understanding of the natural history of familial CRC. However the estimated reduction in risk by removal of precursor advanced adenomas at colonoscopy provides an opportunity for a less-invasive combined strategy using FIT.
In conclusion the authors have developed a compelling rationale for a combined FIT:colonoscopy strategy where previous data has indicated that FIT alone would not be sufficient. Although their study did not identify differences according to levels of CRC risk, further refinement of risk estimates and investigative strategies may facilitate risk-stratified mixed-modality surveillance strategies.
https://www.gastrojournal.org/article/S0016-5085(24)05458-1/pdf
Ciara shares how knowledge of her Lynch Syndrome status enabled her to avail of risk-reduction measures that prevented endometrial cancer
We wish to thank Ciara for allowing us to share her story for World Gynaecological Oncology Day. Ciara hopes by sharing her story she can raise awareness of the role genetic risk-factors play in the development of gynea cancers and give hope to others 💜
Over the years, I was aware of Lynch syndrome due to several members of my Mum’s family having it. My great aunt had wrote out a family tree of all family with the inherited gene. That valuable information was then transferred to the genetics clinic.
After a blood sample in 2017, the genetics clinic confirmed that I had Lynch Syndrome with MSH2 gene alteration. It was recommended that I go for a colonoscopy every two years.
Two years ago I was referred to the Gynaecology department for surveillance. Blood tests, ultrasound tests and endometrial biopsies were offered. It was then I started to research the lifetime risk of endometrial cancer associated to MSH2 (40-60%) and understand the importance of surveillance. My endometrial biopsy confirmed I had atypical endometrial hyperplasia which is a pre-cancerous condition of the uterus. Having risk reducing surgery at 44 was the only and logical thing to do my situation. It has been a lot to process emotionally at times, but I am fortunate to have a loving partner, friends, family and other outlets for support. Under the exceptional care of Dr Astbury and her team at UHG, I had a full abdominal hysterectomy in February this year and have recovered well. I am very lucky the endometrial biopsy surveillance was done when it was. The early detection prevented me from needing further treatment after my surgery. I will be forever grateful for everything Dr Astbury and her team have done in order to protect my health.
Ciara Donoghue
#WorldGODay2024 #GynaeCancers #riskfactors #earlydetection #HereditaryCancers #CancerGenetics
Knowing your family history

Knowing your family history of cancer is a critical aspect of cancer prevention and early detection.
Many types of cancer, including Lynch syndrome-related cancers, have a hereditary component. This means that individuals with a family history of cancer may be at increased risk for developing the same or related types of cancer.
The more you know about your family’s cancer history, the better equipped you will be to make informed decisions about your own health and to take proactive steps to reduce your risk of cancer.
Health Information Bill 2024
Aims to improve the use of health information in Ireland. Health information is generated every time a patient interacts with a health service. For example, when a person sees a doctor or nurse, the details that are recorded become health information. How this information is used is key to supporting integrated care. The right information needs to be available in the right place, at the right time, to ensure the best care and treatment for patients.
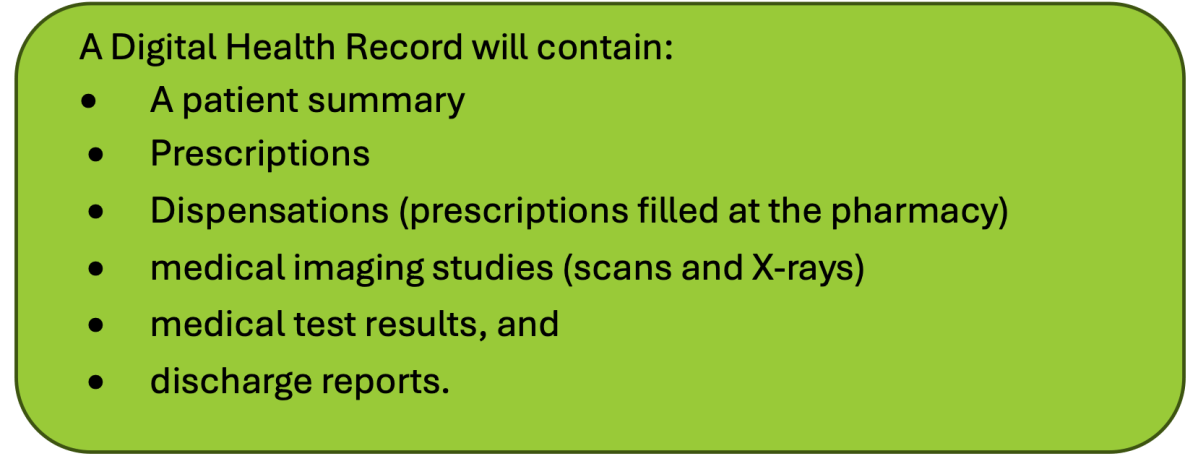
The Health Information Bill helps to achieve this-has a priority focus on digital health records and primary use.
Purpose of the Bill:
Provides for the following in Irish law:
- A ‘duty to share’ health information for patient care and treatment
- The establishment of Digital Health Records for all patients in Ireland
- Greater patient access to their own health information
- Greater protections around health information for primary use
- Better health information for the HSE for public-interest purposes.
AI tools…do we need to be cautious?
PACE-NODES study -(prostate cancer)

The PACE-NODES study for patients with Prostate Cancer is now re-opened at three sites in Ireland.
About this trial
The purpose of this study is to test an advanced type of external beam radiotherapy called stereotactic body radiotherapy (also known as SBRT) in 536 participants with high risk localised prostate cancer (that is, prostate cancer that has not spread beyond the prostate gland but is at high risk of growing quickly or spreading).
Importantly, this treatment delivers a potentially curative dose of radiotherapy in only 5 treatments over two weeks. Half the participants in the trial will receive radiotherapy to the prostate, the other half will have radiotherapy to the prostate as well as the surrounding lymph nodes. The investigators will follow patients in the trial for at least three and half years to see which treatment is best. The investigators will be looking at whether it is safe to give this treatment by reviewing any side-effects that occur and also assessing whether giving SBRT to the lymph nodes as well as the prostate reduces the chance of prostate cancer returning.
