
UCAN Ireland led a broad coalition to call on Minister for Health Jennifer Carroll MacNeill to act now, before Ireland is left with a gap in strategic direction for cancer care.
Cancer cases in Ireland are projected to grow by 47% by 2040, the second-highest projected growth rate in the EU. We cannot afford any gap in strategy or funding.
Our ask is simple:
✅ Commission a formal evaluation of the current strategy immediately
✅ Announce a cancer strategy steering group with meaningful patient involvement
✅ Publish a clear development timeline, with a target publication date no later than end of 2027
✅ Confirm there will be no gap in strategic direction or funding
Blog
The public are not recipients of digital healthcare, but equal stakeholders….
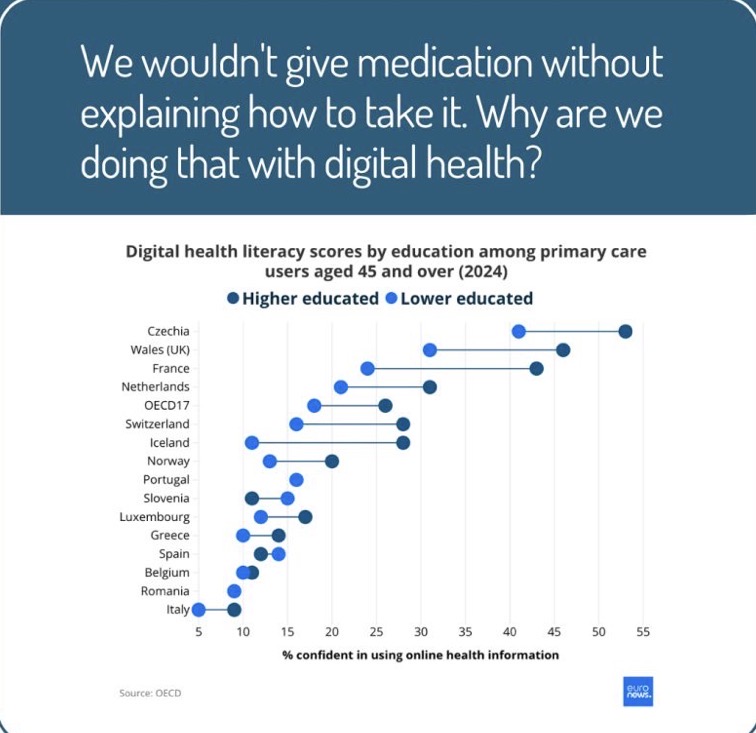
If we focus on merely information sharing or a technology sales pitch, we’ll miss an opportunity to build lasting engagement at the volume required to ensure we can meet everyone’s needs as part of change.
Digital healthcare will succeed if it is built directly with the people it is intended to serve
The symptoms nobody warns you about❗️

When people think about cancer treatment, they often think about #chemotherapy.
But far fewer people talk about digestive issues, unexpected weight loss, food anxiety, pancreatic enzyme replacement (PERT) or the embarrassment that can come with symptoms many patients feel they have to hide.
These are the realities that can have just as much impact on quality of life, yet they’re often left out of the conversation.
If you’ve been affected by a cancer diagnosis – as a patient, carer, or healthcare professional –what symptom do you think deserves more attention❓
Let’s start the conversations that help others feel less alone.
Pamela Deasy(LinkedIn)-Patient Advocacy Pancreatic Cancer Patient Advocate | MA Sociology Student | Turning lived experience into research, awareness, and change
The Unrealised Potential of Cascade Testing
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2850967
The article discusses cascade genetic testing, which means offering genetic testing to close relatives of someone who has already been found to carry an inherited disease-causing gene mutation. e.g. Lynch Syndrome
The idea is simple: if one person has a harmful inherited gene linked to cancer, their parents, siblings, and children may also have it. Finding these relatives early allows them to take steps to prevent cancer or detect it at an early, more treatable stage.
What did the study find?
The researchers looked at nearly 23,000 people who were found to have an inherited cancer-related gene mutation.
The disappointing finding was:
- Only about 24% (roughly 1 in 4) had even one family member go on to have genetic testing.
- That means more than 3 out of 4 people had no relatives tested, despite relatives potentially being at high risk.
The real number may be slightly higher because the study only counted relatives tested through the same laboratory.
The study shows that cascade genetic testing is not reaching enough families. Even when testing is free, most at-risk relatives are never tested. Improving communication, reducing social and cultural barriers, and developing better systems for notifying families could help identify more people at risk and ultimately save lives through earlier detection and prevention of inherited cancers.
‘Less is More’ vs ‘More is More’
Patients Surgical Journey: strategies for patients living with dMMR/MSI CRC. To benefit patients, advance scientific understanding and aid next trial designs, a Multidisciplinary Team approach is essential.
🔍 Key insights discussed include:
• Early-stage dMMR/MSI-H colon cancers are highly immunogenic, making them particularly responsive to checkpoint inhibitor therapy
• The NICHE-2 trial reported remarkable outcomes with neoadjuvant nivolumab plus ipilimumab, including 97% major pathologic response and 67% pathologic complete response rates
• New phase III studies, including AZUR-2 and NeoShot III, are evaluating whether perioperative immunotherapy can improve long-term outcomes compared with current standards
• ctDNA is emerging as a promising biomarker to identify molecular response, guide treatment duration, and potentially support de-escalation of therapy
• Accurate MMR/MSI testing and high-quality radiologic staging are essential when selecting patients for neoadjuvant immunotherapy
• As outcomes continue to improve, future strategies may allow less treatment, fewer surgeries, and more personalized care for selected patients
These data highlight a rapidly evolving treatment paradigm, where biomarker-driven neoadjuvant immunotherapy may transform the management of localised MSI-H colon cancer.
Genitourinary Syndrome of Menopause (GSM)
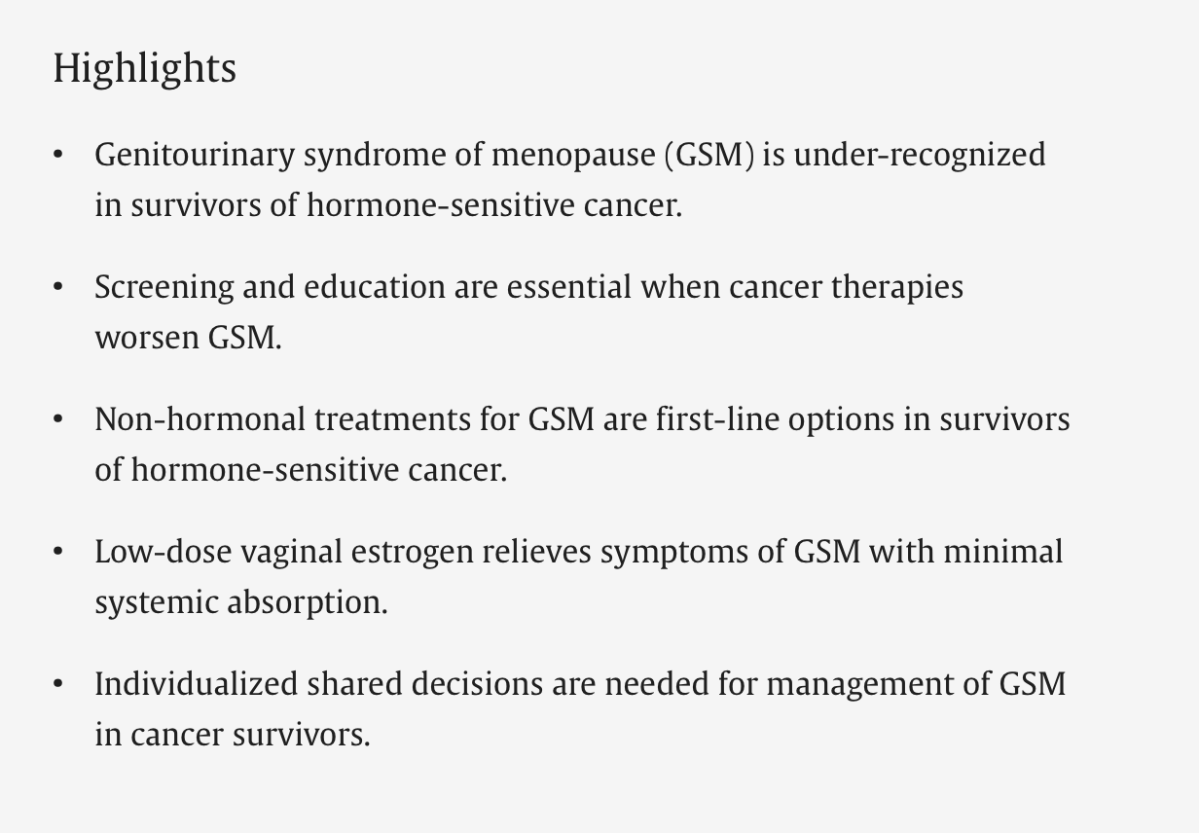
Genitourinary Syndrome of Menopause (GSM) is a common, progressive condition caused by dropping estrogen levels during and after menopause. It affects the tissues of the vulva, vagina, and lower urinary tract, leading to symptoms like vaginal dryness, painful intercourse, urinary urgency, and recurrent urinary tract infections (UTIs).
“Recently published this paper outline the evidence supporting the use of vaginal estrogen to treat (GSM) in women living with or after cancer.
Unfortunately this is an area that is often neglected by clinicians and patients can find it difficult to raise their symptoms or worries during a consultation.
Ultimately low dose vaginal estrogen is likely to be safe and effective in most women with recurrent UTIs or vulvo vaginal atrophy and a history of cancer, however longer term studies would be very helpful.
In the meantime please don’t be afraid to ask your doctor about symptoms such recurrent cystitis, vaginal pain or dryness or painful intercourse there are treatments available”
Donal Brennan-UCD Professor of Gynaecological Oncology at University- College Dublin. LinkedIn.
https://www.sciencedirect.com/science/article/pii/S0378512226001817
Could taking aspirin halve the risk of bowel cancer?
In this episode, they explore the findings from the landmark CaPP3 trial, hear from a participant living with Lynch syndrome, and discuss how genomics could help shift healthcare from treatment to prevention.
Daily low-dose aspirin may significantly reduce bowel cancer risk in people with Lynch syndrome.
The podcast discusses results from the landmark CaPP3 clinical trial investigating aspirin for cancer prevention.
Earlier research found aspirin could reduce bowel cancer risk in people with Lynch syndrome by around 50%.
Lynch syndrome is an inherited condition that greatly increases the risk of bowel and several other cancers.
Genomic testing can identify people who may benefit from targeted prevention strategies like aspirin therapy.
Prevention is becoming an increasingly important role for genomic medicine—not just diagnosing disease.
Aspirin is inexpensive and widely available, making it a potentially accessible prevention option.
Aspirin is not suitable for everyone because long-term use can increase the risk of bleeding and other side effects.
People should only take aspirin for cancer prevention under medical advice. Regular bowel cancer screening remains essential, even for people taking aspirin.
Family genetic testing can identify relatives who may also have Lynch syndrome and benefit from surveillance and prevention.
The podcast highlights how combining genomics, screening, and preventive treatments could improve long-term health outcomes
https://www.genomicsengland.co.uk/podcasts/could-taking-aspirin-halve-the-risk-of-bowel-cancer
Virtual Ward ANP service at St. Vincent’s University Hospital
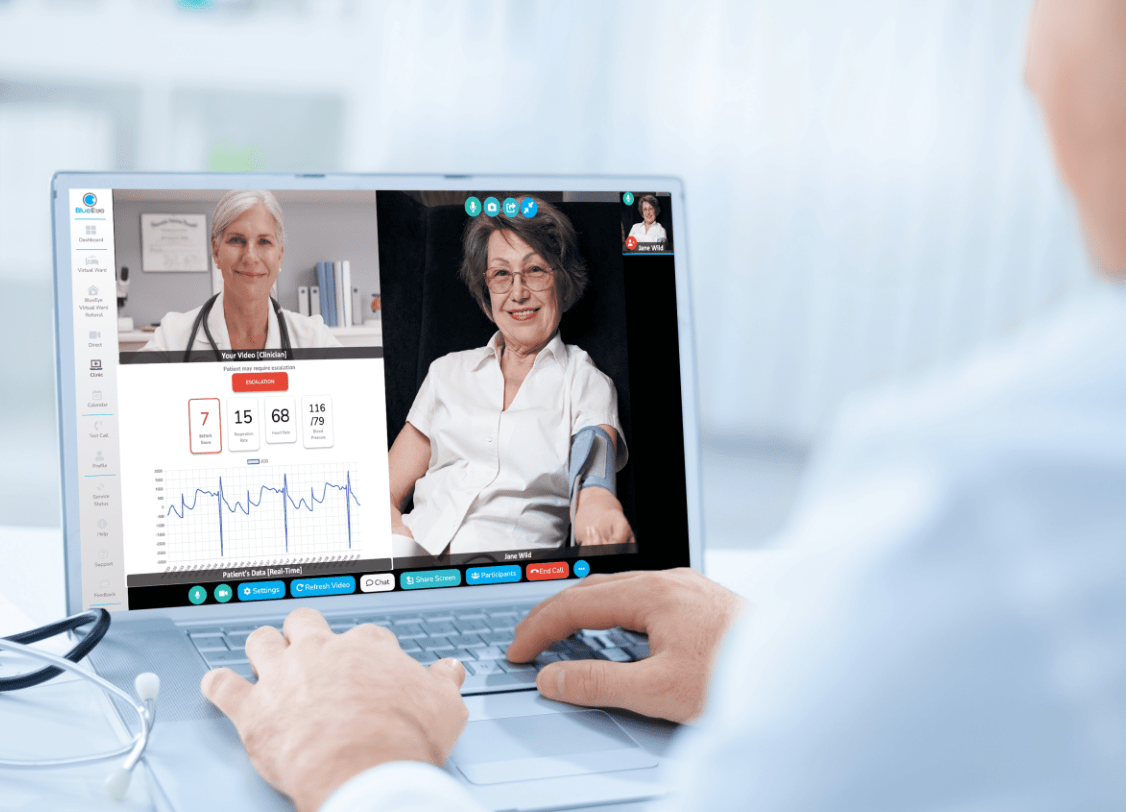
Elaine Whyte, a Registered Advanced Nurse Practitioner (ANP) in the Virtual Ward at St Vincent’s University Hospital in LinkedIn….
Elaine describes the Virtual Ward as an innovative model of care that delivers hospital-level treatment to suitable patients in their own homes through comprehensive clinical assessment, remote monitoring, prescribing, diagnostics, and multidisciplinary teamwork. The service has expanded to include home intravenous therapy, enabling more patients to receive complex treatments without hospital admission.
She emphasises that the greatest benefit of the Virtual Ward is the positive impact on patients, who can recover in familiar surroundings with their families while maintaining independence. Elaine attributes the success of the service to the dedication of a highly collaborative multidisciplinary team and the mentorship she has received throughout her career, highlighting how empowered nursing leadership can transform healthcare delivery.
“Reform must be evident in people’s experience of our health service.”
The newly appointed Derek Tierney , Secretary General of the Irish Department of Health, has set out this important principle.
Patient experience is shaped by how the organisation itself functions.
When accountability is clear, decisions are owned, delays are challenged and learning is visible, patients and staff experience the difference.
How will patients know when reform is working?
If patient experience is to become the defining measure of reform, then access, safety, outcomes, dignity, complaint resolution and patients’ rights should become visible, published measures of success.
𝐖𝐡𝐞𝐧 “𝐖𝐞 𝐃𝐨𝐧’𝐭 𝐊𝐧𝐨𝐰” 𝐈𝐬 𝐭𝐡𝐞 𝐌𝐨𝐬𝐭 𝐑𝐞𝐬𝐩𝐨𝐧𝐬𝐢𝐛𝐥𝐞 𝐀𝐧𝐬𝐰𝐞𝐫 𝐢𝐧 𝐆𝐞𝐧𝐨𝐦𝐢𝐜𝐬
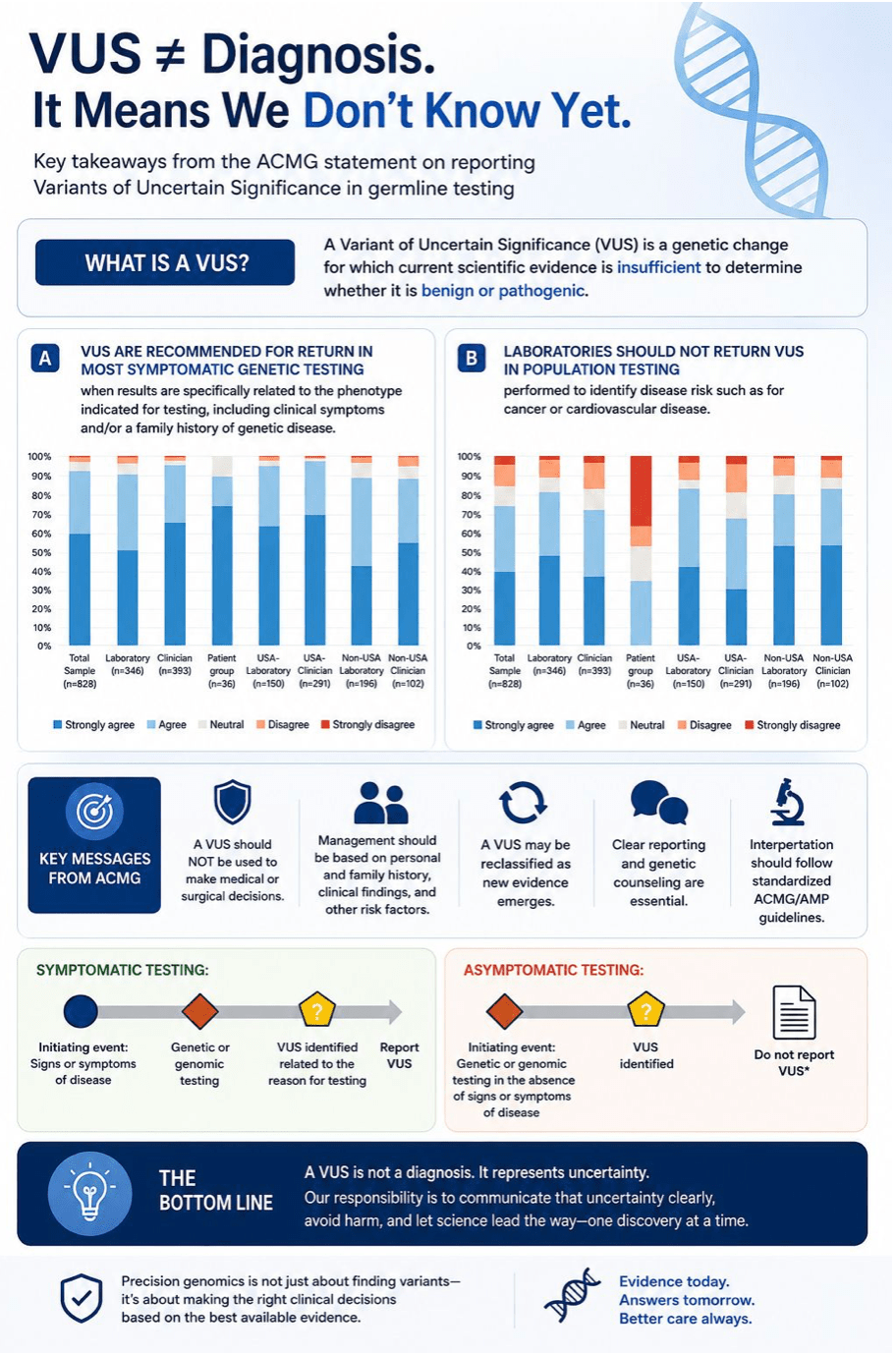
A Variant of Uncertain Significance (VUS) is one of the most misunderstood outcomes in genetic testing.
It doesn’t mean a person has a disease, nor does it mean they are disease-free-it simply means that current scientific evidence is insufficient to determine whether the variant is benign or pathogenic.
The recent American College of Medical Genetics and Genomics (ACMG) statement reinforces several important principles:
✅ A VUS should not be used to guide medical or surgical decisions.
✅ Clinical management should be based on the individual’s personal and family history, not on a VUS alone.
✅ As scientific knowledge grows, a VUS may be reclassified over time, highlighting the importance of periodic review.
✅ Clear communication between laboratories, clinicians, and patients is essential to avoid misinterpretation.
As genomics becomes increasingly integrated into healthcare, understanding the difference between finding a variant and understanding its clinical significance is more important than ever.
Genetics isn’t just about finding answers—it’s also about knowing when the evidence isn’t there yet. “Dr. Jiny Nair-LinkedIn”
