Category: Genetic Testing

GeNotes

The new Gastro-Hepatology collection joins existing specialties such as endocrinology, oncology and neurology, and has been developed by leading experts in gastroenterology and hepatology, including Dr Kevin Monahan, Professor Guruprasad P Aithal and Dr Robert Scott. This collection aims to meet a wide spectrum of genomics education needed for these specialist communities – from when and how to order genomic testing for a patient with a family history suggestive of Lynch syndrome to the underlying genomics at play in hereditary pancreatitis.
https://www.genomicseducation.hee.nhs.uk/news/new-in-genotes-gastro-hepatology/
CANCER TEST DESIGNED BY NEWCASTLE SCIENTISTS COULD IMPROVE SURVIVAL RATES
Lynch syndrome significantly increases a person’s risk of developing certain types of cancer, in particular colorectal which is the fourth most common cancer in the UK.
Screening for Lynch syndrome means that if a person tests positive, a DNA test can then be offered to their relatives to see who else has the condition, so that they can then be put on a regular programme of checks.
The test can also guide the best treatment to provide, as it can indicate whether a person will respond to immunotherapy, a new and effective approach to cancer treatment with increased accuracy.
Newcastle upon Tyne Hospitals NHS Foundation Trust is leading the rollout of the project and the test is being evaluated for patients at the Royal Marsden Hospital, Manchester University NHS Foundation Trust, Birmingham NHS Foundation Trust and Bristol NHS Foundation Trust.
What is genomics?
Is the study of an organism’s genome – its genetic material – and how that information is applied. All living things, from single-celled bacteria, to multi-cellular plants, animals and humans, have a genome – and ours is made up of DNA.
New report highlights UK-wide picture for people affected by Lynch syndrome

Identifying people with Lynch syndrome has important implications for the person affected, and their family members. It is also a crucial part of the puzzle to improve survival of bowel cancer, through increasing early detection in people with a high risk of developing the disease.
Since 2018, considerable progress has been made, with 90% of UK bowel cancer
patients being tested for Lynch syndrome in 2022/23. However, significant challenges with testing family members and offering routine surveillance colonoscopies still require urgent attention.
Testing all newly diagnosed bowel cancer patients for Lynch syndrome (also called universal testing) and routine surveillance are vital to meeting the early diagnosis ambitions set out by governments and health services across the UK.
What is Cascade Genetic Testing?
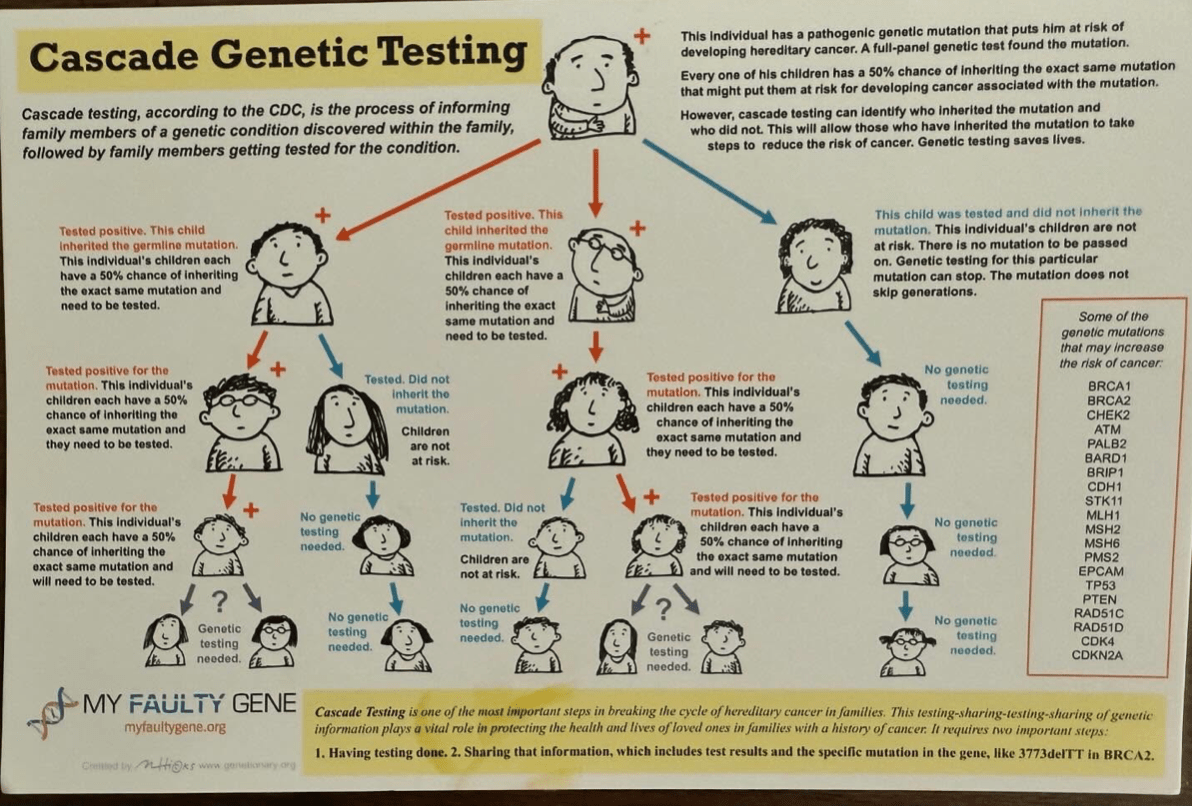
Is the process of informing family members of a genetic condition discovered within the family, followed by family members getting tested for the condition.
It can identify who inherited the mutation and who did not. This will allow those who have inherited the mutation to take steps to reduce the risk of cancer. Genetic testing saves lives.
Cascade Testing is one of the most important steps in breaking the cycle of hereditary cancer in families. This testing-sharing-testing-sharing of genetic information plays a vital role in protecting the health and lives of loved ones in families with a history of cancer.
It requires a number of important steps:
1. Having testing done. 2. Sharing that information, which includes test results and the specific mutation in the gene.
In Lynch syndrome mutations in the following genes may increase the risk of cancer: MLH1, MSH2, MSH6, PMS2 and ЕРСАМ.
EPI what?
Epigenetics: Is a way of influencing how our genome is regulated without the DNA code itself being changed. Epigenetics can determine when genes are turned on and off (also referred to as gene expression), and which proteins are produced as a result. It can even control the structure of the genome, relaxing the tightly packed chromosomes to allow the factors which control gene expression access to the genes within.
One example of an epigenetic modification is methylation, which is associated with switching genes off. Here, a chemical called a methyl group attaches to a region near the start of a gene and prevents it from being switched on.
Lynch syndrome also illustrates the significance of the epigenetic component in cancer development. Inactivation of tumor suppressor genes by epigenetic mechanisms is an acquired property of many tumors developing in Lynch syndrome.
https://www.genomicseducation.hee.nhs.uk/education/core-concepts/what-is-epigenetics/
Neoadjuvant immunotherapy for locally advanced/metastatic mismatch repair deficient colorectal cancer: a two-year institutional experience.

Loss of MMR functioning, termed MMR deficiency (MMRd), leads to microsatellite instability (MSI),2 a hypermutated phenotype, and increased cancer susceptibility. Lynch syndrome patients are at an increased risk for a number of different malignancies, but most commonly develop colorectal and endometrial cancer.
Findings add to the growing body of evidence in support of neoadjuvant immune checkpoint inhibitors for MMRd CRC, and highlight the importance of screening all CRC for MSI-H/ MMRd.
Influence of preoperative Lynch syndrome diagnosis on surgery in patients with colorectal cancer.
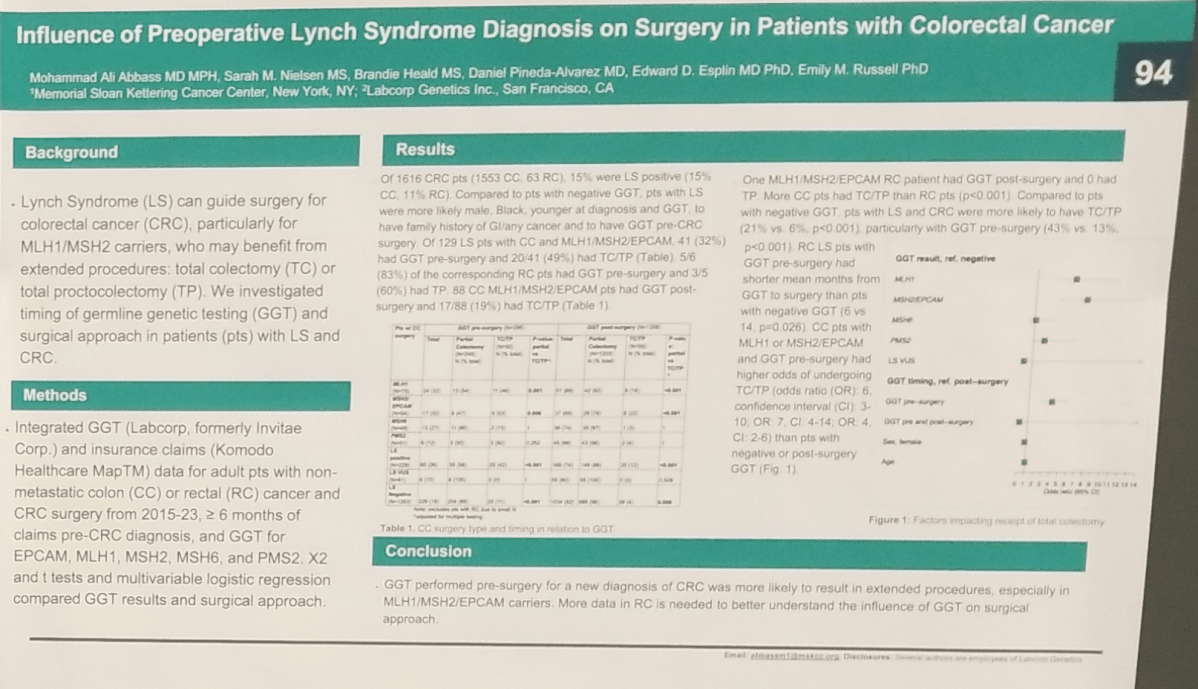
Lynch Syndrome (LS) can guide surgery for colorectal cancer (CRC), particularly for MLH1/MSH2 carriers, who may benefit from extended procedures: total colectomy (TC) or total proctocolectomy (TP).Investigated timing of germline genetic testing (GGT) and surgical approach in patients (pts) with LS and CRC.
Conclusions: GGT performed pre-surgery for a new diagnosis of CRC was more likely to result in extended procedures, especially in MLH1/MSH2/EPCAM carriers. More data in RC is needed to better understand the influence of GGT on surgical approach.
Know your family history

Many men with cancer in the family worry that they are at greater risk of getting it themselves. But this isn’t the case for most people. Cancer is a common disease among older people, so most families will include at least one person who has had cancer.
The more relatives who have had cancer, and the younger they were at diagnosis, the stronger your family history. You may have a strong family history if any of these situations apply to you:
- More than two close relatives on the same side of your family have had cancer.
- The cancers developed when they were young (under the age of 50).
- One of your relatives has had a gene fault found by genetic tests.
5 – 10% of cancers are linked to an inherited gene fault.
What should I do if I have a family history of cancer?
Talk to your doctor who can help you find out if your family history of cancer is of concern. Your doctor may suggest that you visit regularly for screening. In this way, you can pick up problems early.
