
The GENE-ONC Education programme will support healthcare providers and cancer patients by integrating the study of a person’s genes (Genomics) into routine cancer care through both undergraduate and continuing education programmes. Genomic information and data are increasingly used to inform diagnosis and the choice of treatment strategies supporting much more tailored approaches to the management of cancer.
Blog
Genotes – a ‘just-in-time’ genomics education resource co-designed with clinicians

Have you heard about #GeNotes? Flagship resource of NHSE
designed to support clinicians in requesting and managing complex genomic tests – read all about it!Powerful new genomic technologies are transforming the way healthcare is delivered, shaping medical practice across all specialties. In this rapidly changing landscape, there is an urgent need to equip the clinical workforce with knowledge and skills to navigate the new healthcare terrain.
They describe the co-design and co-creation of the GeNotes genomic education resource by clinicians, for clinicians. We anticipate that this approach will have relevance and utility for other educators attempting to meet the needs of a diverse set of end-users in similarly fast-moving fields.
https://link.springer.com/article/10.1186/s12909-024-06059-w
Caregivers

Another incredible example of dedication, compassion & tireless efforts of a caregiver providing essential support to loved ones with #LynchSyndrome
Lynch Syndrome Ireland

Central point for Lynch syndrome related issues in Ireland. An inherited predisposition to certain types of cancer e.g. colon and endometrial.
Bluesky: @lsireland.bsky.social
Instagram: Lynch syndrome Ireland
The Vanishing “Social” in Social Media: The Illusion of Connection

It seems paradoxical, but social media might be making us less social. While we scroll through endless feeds, are we really connecting with others or just consuming content?
So, what about you? Do you feel more connected or isolated when you use social media? Are you building relationships or just consuming content?
Here’s how to spot early signs of prostate cancer

It’s easy to assume that prostate cancer is a disease that only affects older men. But it can strike at any age, including younger and middle-aged men. Although the average age of diagnosis is 68, about one in ten new cases are in men under 55. In fact, doctors have noticed more cases in younger men in recent years. If you’re in your 40s or 50s, it’s worth knowing about the risks and signs of prostate cancer.
Estimated 1 in 7 at risk thorughout their lifetime.
If you’re worried about any symptoms or about your risk of prostate cancer, don’t hesitate to talk to your doctor. Being proactive about your health is important. Remember, many men diagnosed with prostate cancer go on to live long, full lives, especially when it’s caught early.
https://www.rte.ie/brainstorm/2024/1111/1480273-prostate-cancer-risks-signs-symptons-mri-scan/
Improving Patient Comprehension Through Explanatory Communication
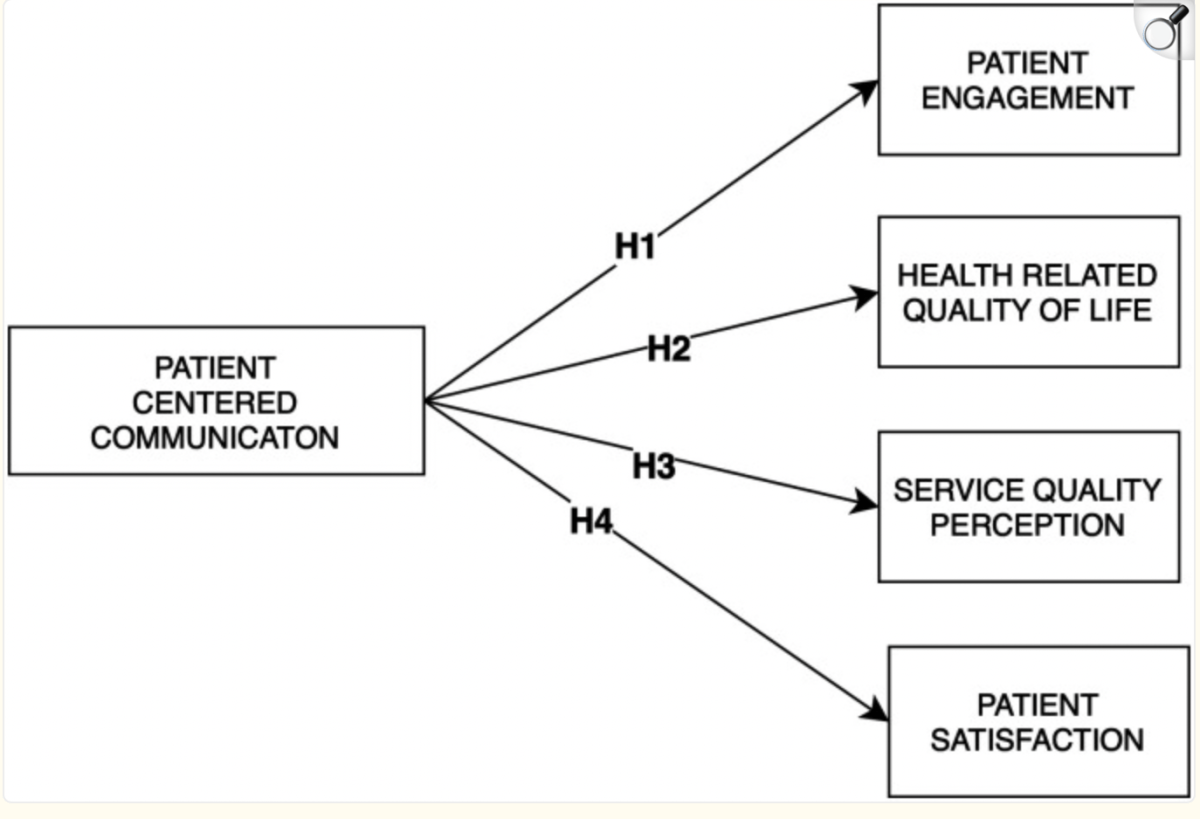
Communication between adult patients with cancer and their health care providers is an important factor in the overall health care experience, contributing to patients’ engagement in treatment, satisfaction with treatment and health care, positive perceptions of health care quality, and ultimately influencing numerous health behaviours and outcomes.
It is important to examine the communication experiences of patients with cancer and the quality of the communication relationship with the service provider, to improve the communication skills of the patient and the service provider, to present patient-centered communication as an integral part of patient-centered care in health systems, and to improve health outcomes by embedding a patient-centered communication perspective.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10901059/#sec23-10732748241236327
Restricted access to effective anti-cancer drugs
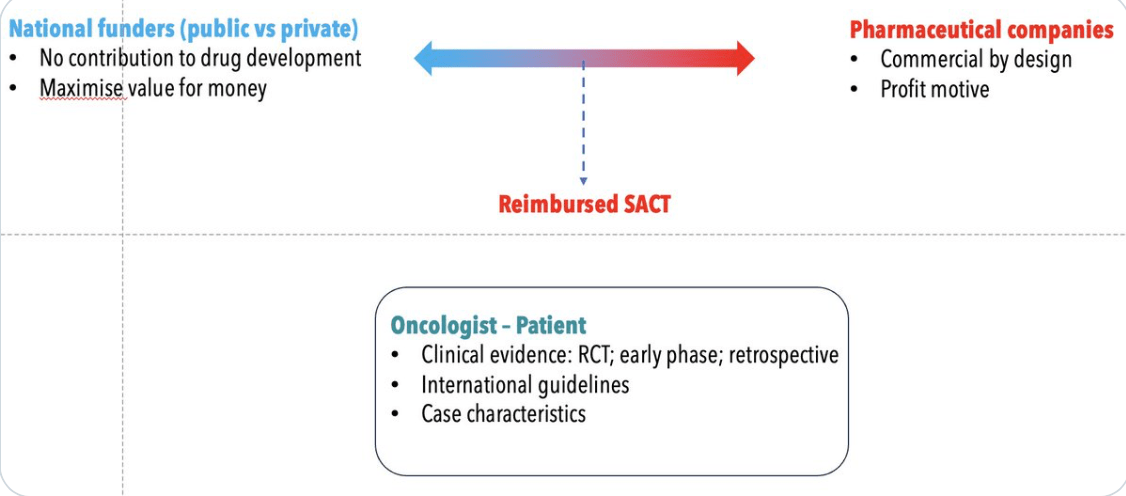
Almost all new ‘cutting edge’ or practice changing cancer therapies are developed commercially, by private companies. This is deliberate, even strategic, on behalf of the public sector.
Not cost-effective does not mean not effective.
Is the Two-tier system failing patients?
https://twitter.com/mccarthymt7/status/1860385822953902315
“Private patients have swift access to European Medicines Agency (EMA) approved anti-cancer drugs, the charity said.
However public patients must wait on average two years to find out if they will get access to the same drugs.” Irish Cancer Society
https://www.rte.ie/news/health/2024/1122/1482285-cancer-health-funding/
Mainstreaming cancer genetics: feasibility of an advanced nurse practitioner-led service diagnosing Lynch syndrome from colorectal cancer in Ireland

Conclusion: Access to and timely delivery of specialist cancer genetics services represents a substantial unmet need in Ireland, the requirement for which is projected to increase significantly over the coming years. Our institutional experience confirms the feasibility, efficiency and efficacy of an ANP-led mainstreamed model of care for hereditary colorectal cancer. The development of this service aligns with national healthcare priorities to deliver timely and appropriate cancer genetics services in a coordinated way integrated with the patient’s cancer care pathway. Development and expansion of similar services would facilitate enhanced delivery of cancer genetics services into routine clinical practice, ensuring uniformity, safety, high quality, and cost-effective care. However, this will necessarily require appropriate resourcing and investment.
Steering the Treatment of Gynecologic Cancers With Biomarkers

Over the past 10 years, PARP inhibitors, immunotherapy and antibody drug conjugates have changed the treatment landscape of gynaecologic cancers, providing options for patients beyond chemotherapy.
Most of the recent FDA approvals for treating patients with gynaecologic malignancies are based on biomarkers. In ovarian cancer, germline genetic testing (patient’s blood or saliva) or somatic profiling (next-generation sequencing of a patient’s tumor) can focus on several biomarkers. For example, it can identify BRCA and homologous recombination deficiency — which occurs in approximately 50% of patients with ovarian cancers and can be treated with PARP inhibitors — and Lynch syndrome, which is a mismatch repair deficiency.
https://www.curetoday.com/view/steering-the-treatment-of-gynecologic-cancers-with-biomarkers
