Very excited to share that @rcsi_irl ‘Patients, Bowels, Basics and Breakthroughs’ is back!!!
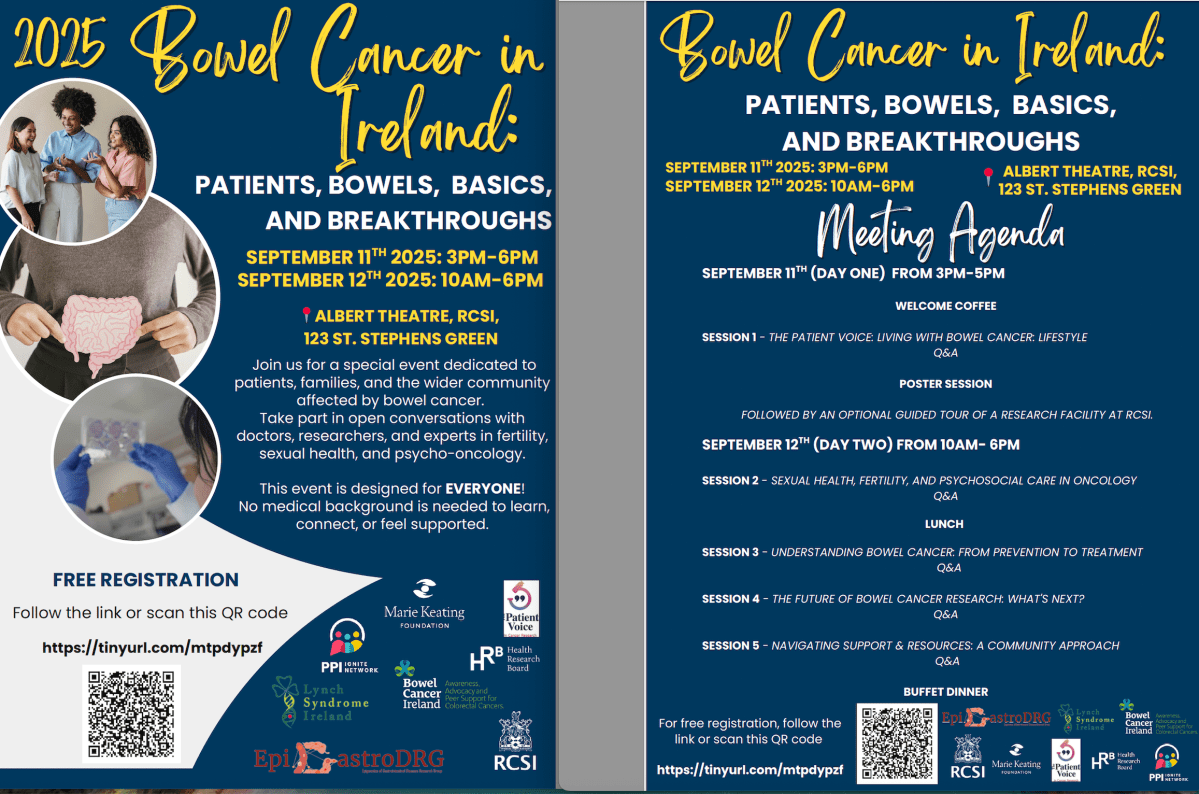
This two day event is aimed at bringing together the patient & professional community to explore the landscape of bowel cancer, with focus on the unique challenges of early-onset disease like fertility, sexual health and much more!
Learn about the latest research directly from those carrying out the work! It will feature fantastic speakers from across Ireland, the UK and Europe and powerful patient voices sharing their lived experiences.
There’ll be exciting panel discussions, a poster session and even a lab tour!
What makes this event even more special is the people behind it. The fabulous (and I mean fabulous!) RCSI Epigastro Disease Research Group who have opened their doors to ourselves at @lynchsyndromeireland & @BowelCancerIreland and welcomed us as valued team members to co-organise these important events. This is more than patient involvement this is true PPI partnership. Together we can do more.
This free event is open to patients and their family members, carers, healthcare professionals and members of the public who would like to learn more about this very common cancer.
When: 11 & 12 September 2025
Where: RCSI St Stephens Green Dublin
Registration is essential. Scan the QR code on poster to register today. Please share the event with anyone who you feel would benefit or be interested.
Let’s talk about bowel cancer, let’s do it all together!